https://youtu.be/lTRlXRFaOXE
Category: Blog
COVID 19 HEART ATTACK DUE TO MICRO-THROMBI IN MICRO-VASCULATURE AND HYDROXYCHLOROQUIN FOR TREATMENT OF COVID 19
COVID 19; SEROPREVALENCE IN DELHI
COVID 19; WHAT IS THE REAL HERD IMMUNITY THRESHOLD ?
https://youtu.be/4qShkavWzvE
The Moderna mRNA VACCINE phase1 published; but WHO will NOT investigate leak from “WIV”
COVID 19 IS NOT MERELY A RESPIRATORY DISEASE.
THE “VIRUS FROM WUHAN” OR THE “WUHAN VIRUS”


Six men entered an abandoned copper mine to clear bat excreta in provide of Yunnan in China sometime in 2012. All six soon became sick with pneumonia and 3 died. Bloods were sent to rule out dengue, Japanese encephalitis, Nipah virus, hepatitis B, hepatitis C and HIV, all turned out negative. It was decided to check for coronavirus antibodies too; this turned out to be positive. Chinese virologists could soon isolate a new coronavirus and named this “RaCoVBT4991.”
By 2018 a new biosafety level 4 lab was ready in the city of Wuhan. Extensive research in bat coronavirus started in this lab. Research in increasing the capacity of coronavirus to latch on to human cells were performed routinely and numerous papers demonstrating “gain of function” were published in leading scientific journals like Science and Nature.
Some of these papers were co authored by American scientists. It was also well known that the US government gave grants for such research in the hundreds of millions of Dollars. Dr.Anthony Fauci was not only aware of these grants but actually facilitated them.

The “gain of function” technique means the combination of bits of genes of different coronaviruses in order to make the recombined new virus more aggressive and infectious. The coronavirus is able to enter human cells by the spikes covering it. These spikes home on to receptor molecules called ACE2. The ACE2 receptors are present in the throat, respiratory passages, heart, kidney, blood vessels, intestine ,liver and also the brain.
Almost all experiments on coronaviruses therefore entailed making the spikes on the virus become more capable of penetrating human ACE2 receptors. One study published explained how a part of the spike making gene in a bat coronavirus was combined with a mouse coronavirus gene, and this new creation had much greater capacity to engage with human ACE 2 receptors, apart from making mice very ill.
The other technique that makes a virus more pathogenic is termed “passaging.” A Dutch team were pioneers in “passaging.” These scientists had the dubious distinction of taking the H5N1 (avian flu) virus and infection a series of 10 ferrets. The procedure required a ferret to be infected by H5N1, then the virus was retrieved from the first ferret and injected into a second ferret and then once again the virus was isolated to be injected into the third ferret, and so on. It was documented that by the time the 10th ferret was infected the H5N1 virus had mutated enough to infect another ferret through air ! The scientists in Amsterdam had made the H5N1 virus airborne.
The H5N1 virus has a case fatality rate of almost 70%. Luckily it is not airborne and is as yet not a human pathogen. It infects humans in close and prolonged contact with chicken. The scientific world was more than a bit alarmed when they learnt that by infecting 10 ferrets one after the other one could convert the H5N1 virus into an airborne one. The ramifications were scary; the Americans suspended all such experiments on enhancing viruses within their shores from 2014 to 2017. During this period they financially supported Chinese scientists to continue with the techniques of making viruses more lethal, under the pretext of making new therapeutics and vaccines.
Interestingly when the Covid-19 Pandemic broke out, the new coronavirus for some very strange reasons was named “SARS-CoV-2” after the coronavirus that caused severe acute respiratory syndrome or SARS in 2012. This now seems very odd because genomic similarity between SARS-2 and SARS-1 is a mere 79%. But similarity of genome with the 2013 Yunnan virus is a whopping 96.2%!
Intriguingly albeit the Chinese scientists mentioned the RaCovBT4991 in their paper on bat coronaviruses, they conveniently never informed the world of its lethality. Remember 3 of 6 people infected had died in 2013 after being infected by the bat coronavirus. Also somewhere down the line the Chinese renamed RaCovBt4991 to RaTG13. We will hence focus our attention on RaTg13.
A paper was published 4 days ago in Nature by a group from the UK that compared infectivity of so called SARS-CoV-2 with RaTg13. The researchers concluded that the virus causing the current havoc across the planet is 1000 times more capable of latching on to human ACE 2. The chances of a virus with 96.2% genomic similarity to mutate within only 8 years to the new coronavirus are extremely remote. Such a mutation would normally take more than 5 to 7 decades at least. There is therefore human hand at play here, which has made the spikes of the Pandemic virus ferociously aggressive and infective.
I would be inclined to rename SARS-CoV-2 to something else only based upon its genetic characteristics.
PublishedOnline
June 25, 2020 https://doi.org/10.1016/ S2215-0366(20)30287-X
Also SARS (caused SARS-CoV-1) presents with fever , body aches and pneumonia. The clinical presentation was restricted to thesis features. The 2019 coronavirus, however, manages to attack multiple other organs. For instance the brain can be affected without pneumonia. Patients may have stroke or even severe psychiatric changes. Inflammation of the brain can be confirmed by a brain MRI or presence of the virus in the CSF. A paper including 150 such patients has already been published.
Almost a third of serious patients admitted in intensive care have been found to have cardiac abnormalities. These patients have raised troponin levels, and impaired heart function. There may be patients who have acute myocarditis (inflammation) without any fever or pneumonia. Myocarditis has been confirmed by heart MRI. Causation of myocarditis is confirmed by ruling the role of other viruses such as HIV, Hep B,Hep C, cardiotropic virus and Lyme disease. Covid-19 was confirmed by the PCR test.

Patients may suffer heart attack directly by the new corona virus which destabilises the plaque in the coronary artery or indirectly by increasing work load of the heart , and also by making the blood more coagulable. These changes may be sen in absence of pneumonia; hence an astute clinician will always be on the look out for the new coronavirus when confronted with a heart attack, irregular rhythm, or heart failure.

Almost 35% patients admitted in New York hospitals had acute kidney injury and 14% needed dialysis. This virus can directly attack kidneys or compromise blood vessels supplying them.
Autopsies have confirmed the presence of a diffuse vasculitis or inflammation of medium and small sized blood vessels. Endotheliitis has been seen in vessels of almost organs. Infallmation of blood vessels leads to small and big blood clots that amplify the disease and worsen prognosis. Empirical low molecular weight heparin is advised but effectiveness is unknown.
The new coronavirus can directly destroy pancreas cells that produce insulin and also indirectly by interleukin 6 (IL6) , which is a pro inflammatory protein. This results in raised blood sugar demanding more insulin in patients with diabetes. Blood sugar can also be found increased in patients with previously normal blood sugars.
Anti-diabetes treatment should ideally be insulin , because almost all other drugs may impair other organs. Sulfonylureas for example may affect cardiac function, while SGLT2 inhibitors may play havoc with kidneys or create ketosis.
The reason I have enumerated the different organs affected by Covid 19 is to make clear that this disease is clinically far removed from SARS. There is little clinical resemblance to SARS and therefore the current given name of the new coronavirus is quite illogical to say the least.
It should be emphasised that multisytem involvement is seen in the minority of patients admitted in intensive care. The majority of patients have mild or no symptoms. Also fatality rate in India is amazingly lows compared to Western nations; new cases per day in Delhi have been steadily falling since June 23rd from 4000 a day to 1250 2 days ago.
The new virus bears little genomic resemblance to SARS, and also has distinct clinical characteristics. It therefore should be renamed. This may not be politically correct but we do have the “Delhi belly”or the travellers’ diarrhoea. The WHO has or will be dispatching a fact finding mission of an epidemiologist and an animal health expert to confirm whether this new virus originated from an animal. Curiously, the Wuhan Institute of Virology will not be investigated.
The new coronavirus should not be called SARS-CVoV-2. A much more appropriate name would be the “Yunnan Virus” or the “Wuhan Virus.”
COVID 19:THE INDIAN (ICMR) VACCINE TO BE LAUNCHED BY 15th AUGUST 2020
https://youtu.be/lhJfX-o5itI
The ministry of health and the Indian Council of Medical Research have despatched an astounding letter to “Dear colleagues” to “envisage ” public health use of the Indian vaccine no later than 15th August 2020, “after completion of all clinical trials.” The letter goes on to warn the recipients that “non-compliance will be viewed very seriously.” Obviously all science has been thrown to the winds on demanding a vaccine for public health use latest by 15th August 2020. The tenor of the letter is more in the realm of extortion than scientific communication.
A vaccine like any new drug mandates 3 phases of clinical trials ; phase 1 to assess safety, phase 2 to check efficacy and then a phase 3 trial in tens of thousands of participants to check for both safety and efficacy. The 3 phases just CANNOT be done in 5-6 weeks.
The health secretary could be pardoned because he obviously has no idea of vaccines or clinical trials, but for the director general of the Indian Council of Medical Research to pen such a letter is laughable.
References:-
1)ChAdOx1 nCoV-19 vaccination prevents SARS-CoV-2 pneumonia in rhesus macaques bioRxiv preprint doi: https://doi.org/10.1101/2020.05.13.09….
2)Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine:a dose-escalation, open-label, non-randomised, rst-in-human trial. Lancet 2020; 395: 1845–54
3)Trial of Moderna Covid-19 vaccine delayed, investigators say, but July start still possible By Damian Garde @damiangarde. STAT, July 2, 2020
4)Doubts over Oxford vaccine as it fails to stop coronavirus in animal trials. The Telegraph 18 May 2020.
COVID 19 :WAS THE VIRUS LEAKED FROM WUHAN INSTITUTE OF VIROLOGY?
Tweaking or tinkering with the beta coronavirus is not very difficult. Numerous papers published in peer reviewed scientific journals have reported the techniques of “passaging” and “gain of function.” These techniques can make the bat coronavirus more infective and also more lethal. The Wuhan Institute of Virology is the leading centre for research to increase capability of bat coronaviruses to infect humans. The Americans have pumped in more than $ 7 million into the Wuhan Institute of Virology. No wonder no investigation will ever confirm whether SARS-CoV-2 is “accidental” , “natural” or “deliberate.” Experiments enhancing lethality of viruses MUST STOP immediately.
References:-
1:COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study Lancet Child Adolesc Health 2020 Published Online June 25, 2020 https://doi.org/10.1016/ S2352-4642(20)30177-2
2:Childhood Multisystem Inflammatory Syndrome — A New Challenge in the Pandemic This editorial was published on June 29, 2020, at NEJM.org.
3:Multisystem Inflammatory Syndrome in U.S. Children and Adolescents This article was published on June 29, 2020, at NEJM.org. DOI: 10.1056/NEJMoa2021680
4:Multisystem Inflammatory Syndrome in Children in New York State This article was published on June 29, 2020, at NEJM.org. DOI: 10.1056/NEJMoa2021756
5:Airborne Transmission of Influenza A/H5N1 Virus Between Ferrets 22 JUNE 2012 VOL 336 SCIENCE www.sciencemag.org
6:A SARS-like cluster of circulating bat coronaviruses shows potential for human emergence Vineet D Menachery1, Boyd L Yount Jr1, Kari Debbink1,2, Sudhakar Agnihothram3, Lisa E Gralinski1, Jessica A Plante1, Rachel L Graham1, Trevor Scobey1, Xing-Yi Ge4, Eric F Donaldson1, Scott H Randell5,6, Antonio Lanzavecchia7, Wayne A Marasco8,9, Zhengli-Li Shi4 & Ralph S Baric1,2 VOLUME 21 | NUMBER 12 | DECEMBER 2015 nature medicine
7:A pneumonia outbreak associated with a new coronavirus of probable bat origin 270 | Nature | Vol579 | 12March2020
8:The Re-Emergence of H1N1 Influenza Virus in 1977: A Cautionary Tale for Estimating Divergence Times Using Biologically Unrealistic Sampling Dates PLoS ONE | www.plosone.org 1 June 2010 | Volume 5 | Issue 6 | e11184
9:Coexistence of multiple coronaviruses in several bat colonies in an abandoned mineshaft Xing-Yi Ge1#, Ning Wang1#, Wei Zhang1, Ben Hu1, Bei Li1, Yun-Zhi Zhang2,3, Ji-Hua Zhou2, Chu-Ming Luo1, Xing-Lou Yang1, Li-Jun Wu1, Bo Wang1, Yun Zhang4, Zong-Xiao Li4, Zheng-Li Shi1* VIROLOGICA SINICA 2016, 31 (1): 31–40 DOI: 10.1007/s12250-016-3713-9
10:The possible origins of 2019-nCoV coronavirus Preprint · February 2020 DOI: 10.13140/RG.2.2.21799.29601
11:Dr. Fauci Backed Controversial Wuhan Lab with U.S. Dollars for Risky Coronavirus Research BY FRED GUTERL ON 4/28/20 AT 2:57 PM EDT; NEWSWEEK
12:CORONAVIRUS Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation Wrapp et al., Science 367, 1260–1263 (2020) 13 March 2020 1 of 4
13:Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses NAtuRe MiCRoBioLogy | VOL 5 | MARcH 2020 | 562–569 | www.nature.com/naturemicrobiology
COVID 19: IS TIME TO THINK OF REOPENING SCHOOLS ?
The RT-PCR test is not a foolproof test; therefore the CDC, FDA , and local certified labs add the caveat that a positive test does not exclude infection by another virus or bacteria, also a positive test does not confirm cause of symptoms or disease is SARS-CoV-2. Life must go on, especially in India where mortality by Covid-19 is remarkably low, despite millions being infected. The doomsayers conveniently forget to mention the low death rate in Indians. It is high time serious thought was given to opening of schools , or else a generation of children will have their future seriously dented. Schools are opening up in many countries of the world. There is ample data that children are infected significantly less than adults, if infected they shrugged off the virus admirably well, very few succumb to the disease. Schools are a vital part of a child’s growth, educationally, socially and emotionally. Friendships are made for life and a child gets to realise her or his trajectory in life. Disruption of schools will particularly affect millions of poor children who seem to have no one to speak on their behalf. Online teaching is no match for the classroom, and poor children have no access to the internet.
References:-
1:Protecting the psychological health of children through effective communication about COVID-19 Lancet Child Adolesc Health 2020 Published Online March 31, 2020 https://doi.org/10.1016/ S2352-4642(20)30097-3
2:Mental health considerations for children quarantined because of COVID-19 Lancet Child Adolesc Health 2020 Published Online March 27, 2020 https://doi.org/10.1016/ S2352-4642(20)30096-1
3:Kawasaki-like multisystem in ammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study : BMJ2020;369:m2094 http://dx.doi.org/10.1136 bmj.m2094
4:Research Shows Students Falling Months Behind During Virus Disruptions Published June 5, 2020 Updated June 6, 2020, The New York Times.
5:Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China Cite as: J. Zhang et al., Science 10.1126/science.abb8001 (2020).
6:Short Communication: Submitted to Osong Public Health and Research Perspectives Coronavirus disease-19: The First 7,755 Cases in the Republic of Korea medRxiv preprint doi: https://doi.org/10.1101/2020.03.15.20….
7:Covid-19 outbreak in Vo, Italy medRxiv preprint doi: https://doi.org/10.1101/2020.04.17.20….
8:Age specificity of cases and attack rate of novel coronavirus disease (COVID-19) medRxiv preprint doi: https://doi.org/10.1101/2020.03.09.20….
9:Lockdown is not egalitarian: the costs fall on the global poor June 19, 2020 https://doi.org/10.1016/ S0140-6736(20)31422-7 www.thelancet.com
10:Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: a retrospective cohort study.
11:Lancet Infect Dis 2020 Published Online April 27, 2020 https://doi.org/10.1016/ S1473-3099(20)30287-5
12:School Children Don’t Spread Coronavirus, French Study Shows By Marthe Fourcade June 23, 2020, 6:41 PM GMT+5:30; Bloomberg
13:Determining the optimal strategy for reopening schools, work and society in the UK: balancing earlier opening and the impact of test and trace strategies with the risk of occurrence of a secondary COVID-19 pandemic wave medRxiv preprint doi: https://doi.org/10.1101/2020.06.01.20….
14:Dong Y MX, Hu Y, et al. Epidemiology of COVID-19 among children in China. Pediatrics. 2020.
15:Lu X, Zhang L, Du H, Zhang J, Li YY, Qu J, et al. SARS-CoV-2 Infection in Children. N Engl J Med. 2020.
16:Cai J, Xu J, Lin D, Yang Z, Xu L, Qu Z, et al. A Case Series of children with 2019 novel coronavirus infection: clinical and epidemiological features. Clin Infect Dis. 2020.
17:COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study Lancet Child Adolesc Health 2020 Published Online June 25, 2020 https://doi.org/10.1016/ S2352-4642(20)30177-2
THE PERILS OF MATHEMATICAL MODELS SHOULD HAVE BEEN OBVIOUS.

Finally both The Times of India (18th June 2020) and The Indian Express (19th June 2020) have cited an editorial published by the Indian Journal of Medical Research that all mathematical models on the Covid-19 pandemic were incorrect, and worse carry a “strong element of bias.”
Sadly the edit does not provide any further elaboration on this “bias”. It was expected that the authors dived deep into their “bias” hypothesis. Especially because of the fact that the numbers sprayed by the doomsayers have just not materialised. The exaggeration was so obvious that it took ones breath away. Data from all over the world kept pouring in that mortality in Covid-19 ranged around 1-2 infected per thousand, at times even less than this. But the doom sayers persisted with their doom and gloom predictions as recently as this week.
Astonishingly the doomsayers have been provided platforms by the media all these months. The predictions made for terrifying headlines. The protocol in the media was rapidly established, the bigger the numbers for people infected , the greater would be force the force behind the news stories published and interviews recorded.
Editors scrambled without exception to provide more and more sensational headlines. No one questioned the source of these deeply flawed models. Neither has this editorial. The authors of the editorial need to answer as to why they presume there was a strong bias by the modellers ? What is a weak “bias?” What were the forces behind the “bias?” Does it really matter whether the modellers were from the university of Kurukshetra or the University of Washington? Was there any influence of these modellers with “bias” on the ICMR?
Who funds these newly established non governmental centres for disease control in India? These are some hard questions that need to be checked. Did the media inadvertently provide publicity to these modellers? Or were they hand in glove? Did the editors not realise that despite large-scale infectivity the death rate of the SARS-CoV-2 was very low amongst Indians. As opposed to death rate in Western countries of 3 figures per million, the Indian death rate has been a single digit per million of the population.
As of today there have been 12,605 deaths in India at a rate of 9 per million. A remarkably low number but true. There is always the probability that a considerable number of these deaths may be with Covid-19 virus as a bystander, rather than because of it. The modellers however has predicted lakhs of deaths.
Unfortunately these modellers were taken at face value, and not unlike the rest of the world, the government was compelled to over react. Who wants lakhs of deaths on their watch? Certainly no sane or responsible government. The English government responded to the Imperial college “document” as did we to our own brilliant modellers. The repercussions will be felt far and wide and sadly for a long time.
It is so obvious that lakhs of business lie ruined, lakhs of people were forced to literally walk thousands of kilometres back to their villages. Hundreds succumbed in the ordeal. Little girls walked bare feet hundreds of kilometres to drop dead due to exhaustion and starvation. Many got ploughed down by vehicles as they trudged home in utter despair. The harrowing list of miseries is endless.
But despite the clearly visible and palpable sufferings of lakhs of people the media refused to suspend sensationalism around Covid-19. The interviews kept coming, guests repeated ad nauseam that millions would be infected by SARS-CoV-2. That millions would get infected is so obvious that repeating this fact again and again is downright stupid or deliberate scare mongering.
The number of infected people infected so far are 381,485. Any public health student will know that in reality at least 10 times this number are actually infected. There is considerable serological data from across the globe ascertaining to the fact that at least 10 times more people are infected that those detected by a positive RT-PCR test. We therefore have at least 3.8 million people infected.
3.8 or 4 million people infected seems like a huge number till we bear in mind that we have 1,350 million people in our country. This implies that only 0.296% of our population has been infected by Covid-19. The mainstream and alternate media however keeps drumming the “millions” number.
When you keep repeating the “millions’ figure, knowing very well that as the denominator expands the mortality rate gets lowered there is a strong chance that some agenda is at play. Sensationalism for 4 weeks my be considered an inadvertent error, but to keep flogging a weakening horse over months becomes more than suspicious.
Why an online so called alternative media magazine priding itself on objectivity repeatedly invite doomsayers for interviews is downright baffling if not suspicious. There is neither science nor any substance in the interviews.
I have been repeatedly (in my blogs, videos and interviews ) underscoring the low mortality rate in Covid-19 patients. This was not based on astrology but on painstaking evidence gathered from peer reviewed medical literature. Above all there was absolutely no agenda. It certainly was not for applause or being in the spot light. The panic was becoming both visible and palpable, the ramifications of the fear will cast a large shadow for years to come.
According to the Swiss Policy Research the overall lethality of Covid-19 is about 0.1% as per the latest immunological and serological studies. Thus in the range of a strong seasonal flu.
The overall mortality in in the range of a strong flu season in countries like the UDS,UK, and also Sweden ( without a lockdown). In country like Germany, Austria and Switzerland overall mortality is in the range of a mild flu season.
Upto 80% of test positive cases remain without symptoms. Even among 70-79 year old, about 60% remain symptom free. Almost 95% patients develop moderate symptoms.
Importantly 60% of people may have cellular background immunity to Covid-19 due to previous common colds (coronavirus infection).
The average age of people dying is 80 years and 96% of these have chronic illnesses.
When people sit down to write about these times centuries from now, they surely will notice that more people died of fear of this virus than by the virus itself.
A lot of this fear has been fuelled by the modellers and the media. Mercifully some in the print media have finally realised that the mathematical models presented all these months are manifestly incorrect.
COVID-19 ; TOCILIZUMAB ; THEODORE ROOSEVELT AIRCRAFT CARRIER
https://youtu.be/5ZYmDgAu5Zg
Antivirals can definitely play a role in management of Covid-19 patients. The only 2 drugs with randomised trials so far are Interferon and Remdesivir. Interferon should be given before 7 days of symptom onset. The very few patients that do not recover may need tocilizumab which acts against interleukin-6 receptors.Only one injection may be needed. The aircraft carrier Theodore Roosevelt has demonstrated that 60% of infected patients remain asymptomatic, 60% develop antibodies and above all only 1 sailor succumbed out of the 1100 infected.
Hence case fatality rate is less than 0.1% in young and fit sailors. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: an open-label, randomised, phase 2 trial
Published Online The Lancet; May 8, 2020 https://doi.org/10.1016/ S0140-6736(20)31042-4
Remdesivir for the Treatment of Covid-19 — Preliminary Report
J.H. Beigel, K.M. Tomashek, L.E. Dodd, A.K. Mehta, B.S. Zingman, A.C. Kalil, E. Hohmann, H.Y. Chu, A. Luetkemeyer, S. Kline, D. Lopez de Castilla, R.W. Finberg, K. Dierberg, V. Tapson, L. Hsieh, T.F. Patterson, R. Paredes, D.A. Sweeney, W.R. Short, G. Touloumi, D.C. Lye, N. Ohmagari, M. Oh, G.M. Ruiz-Palacios, T. Benfield, G. Fätkenheuer, M.G. Kortepeter, R.L. Atmar, C.B. Creech, J. Lundgren, A.G. Babiker, S. Pett, J.D. Neaton, T.H. Burgess, T. Bonnett, M. Green, M. Makowski, A. Osinusi, S. Nayak, and H.C. Lane, for the ACTT-1 Study Group Members* This article was published on May 22, 2020, at NEJM.org.
Remdesivir for 5 or 10 Days in Patients with Severe Covid-19
Jason D. Goldman, M.D., M.P.H., David C.B. Lye, M.B., B.S., David S. Hui, M.D., Kristen M. Marks, M.D., Raffaele Bruno, M.D., Rocio Montejano, M.D., Christoph D. Spinner, M.D., Massimo Galli, M.D., Mi-Young Ahn, M.D., Ronald G. Nahass, M.D., Yao-Shen Chen, M.D., Devi SenGupta, M.D., Robert H. Hyland, D.Phil., Anu O. Osinusi, M.D., Huyen Cao, M.D., Christiana Blair, M.S., Xuelian Wei, Ph.D., Anuj Gaggar, M.D., Ph.D., Diana M. Brainard, M.D., William J. Towner, M.D., Jose Muñoz, M.D., Kathleen M. Mullane, D.O., Pharm.D., Francisco M. Marty, M.D.,Karen T. Tashima, M.D., George Diaz, M.D., and Aruna Subramanian, M.D., for the GS-US-540-5773 Investigators*
This article was published on May 27, 2020, at NEJM.org. DOI: 10.1056/NEJMoa2015301
medRxiv preprint doi: https://doi.org/10.1101/2020.05.29.20117358.this version posted June 3, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-NC-ND 4.0 International license . Tocilizumab for COVID-19 Tocilizumab for treatment of mechanically ventilated patients with COVID-19 Emily C Somers, PhD ScM1,2,3*, Gregory A Eschenauer, PharmD4*, Jonathan P Troost, PhD5, Jonathan L Golob, MD PhD1, Tejal N Gandhi, MD1, Lu Wang, PhD6, Nina Zhou, MS6, Lindsay A Petty, MD1, Ji Hoon Baang, MD1, Nicholas O Dillman, PharmD7, David Frame, PharmD4, Kevin S Gregg, MD1, Dan R Kaul, MD1, Jerod Nagel, PharmD7, Twisha S Patel, PharmD7, Shiwei Zhou, MD1, Adam S Lauring, MD PhD1, David A Hanauer, MD MS8, Emily Martin, PhD9, Pratima Sharma, MD MS1, Christopher M Fung, MD10, Jason M Pogue, PharmD4
Effective treatment of severe COVID-19 patients with tocilizumab
Xiaoling Xua,1,2, Mingfeng Hanb,1, Tiantian Lia, Wei Sunb, Dongsheng Wanga, Binqing Fuc,d, Yonggang Zhouc,d, Xiaohu Zhengc,d, Yun Yange, Xiuyong Lif, Xiaohua Zhangb, Aijun Pane, and Haiming Weic,d,2
www.pnas.org/cgi/doi/10.1073/pnas.2005615117
Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in severe patients with COVID-19
S. Sciascia1,2, F. Aprà2, A. Baffa1,2, S. Baldovino1,2, D. Boaro2, R. Boero2, S. Bonora2, A. Calcagno2, I. Cecchi1,2, G. Cinnirella2, M. Converso2, M. Cozzi1,2, P. Crosasso2, F. De Iaco2, G. Di Perri2, M. Eandi3, R. Fenoglio1,2, M. Giusti2, D. Imperiale2, G. Imperiale2, S. Livigni2, E. Manno2,
COVID-19 ;SENSATIONAL HEADLINES; T-CELL IMMUNITY
Newspapers need to desist from sensational headlines; columnists ought to restrict themselves to facts, mortality in India is indeed lower than other countries; probably because of some form of hidden and unknown immunity. The undeniable fact is that few die from Covid-19 in India as compared to other nations. Either one supports extended lockdown or welcomes the easing of lockdown. One cannot demand both in the same breath.
References:-
Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: an international cohort study
Published Online,The Lancet. May 29, 2020 https://doi.org/10.1016/ S0140-6736(20)31182-X
Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection Shaoqing Leia, Fang Jiangb,c, Wating Sua, Chang Chend, Jingli Chene, Wei Meif, Li-Ying Zhana, Yifan Jiaa, Liangqing Zhangg, Danyong Liug, Zhong-Yuan Xiaa,*, Zhengyuan Xiab,c,g,*
EClinicalMedicine. https://doi.org/10.1016/j.eclinm.2020.100331
Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals
Grifoni et al., 2020, Cell 181, 1–13
June 25, 2020 a 2020 Elsevier Inc. https://doi.org/10.1016/j.cell.2020.05.015
https://youtu.be/XmUbSXT7qPE
“LOCKDOWNS ARE A CRUDE POLICY”
Facing the House of Lords , Neil Ferguson, also known now as “Professor Lockdown,” responded that “lockdowns are a crude policy.” A remarkable turnaround. Of course they are , when they shatter the lives of crores of people. After the damage has been done Professor Lockdown advises a more targeted approach would have been more appropriate. The predictions that there would be 20 to 22 lakh deaths in the US, 5 to 8 lakh deaths in the UK and 70,000 to 100,000 in Sweden were dangerously way off the mark. We have the death figures with us , and these are substantially lower than what the models suggested. Sweden has had 4562 deaths, far less than the 70000 to 10000 predicted; and WITHOUT lockdown

When one looks back it is obvious the entire Indian media was deriving great pleasure in publishing interviews with “public health workers” who out did one another in predicting dooms day scenarios. One after the other they came up with astronomical death rates that ran into lakhs of deaths due to Covid-19. The corridors would be full of patients they said. The result is that the Indian public is paralysed with fear. The enlightened “editors” living on a completely different moral pedestal left no stone unturned in amplifying the terror.
One had expected better sense from the “alternate media” in this country, but they turned out to be the biggest culprits. Scare mongering is as natural to them as breathing. The number of deaths by Covid-19 are in dispute but there is little doubt that viewership rocketed directly in proportion to the dread spread.
One can wake up a sleeping person but how do you wake a man who pretends to sleep. The damage is done. Crocodile tears are being copiously shed for the misery of the lakhs who got displaced and lost their livelihoods. There is no need for elaboration, the catastrophe is there for all to see. The contribution of the media to the disaster is immensely worrying. There is some sadistic pleasure in providing death rates every day.
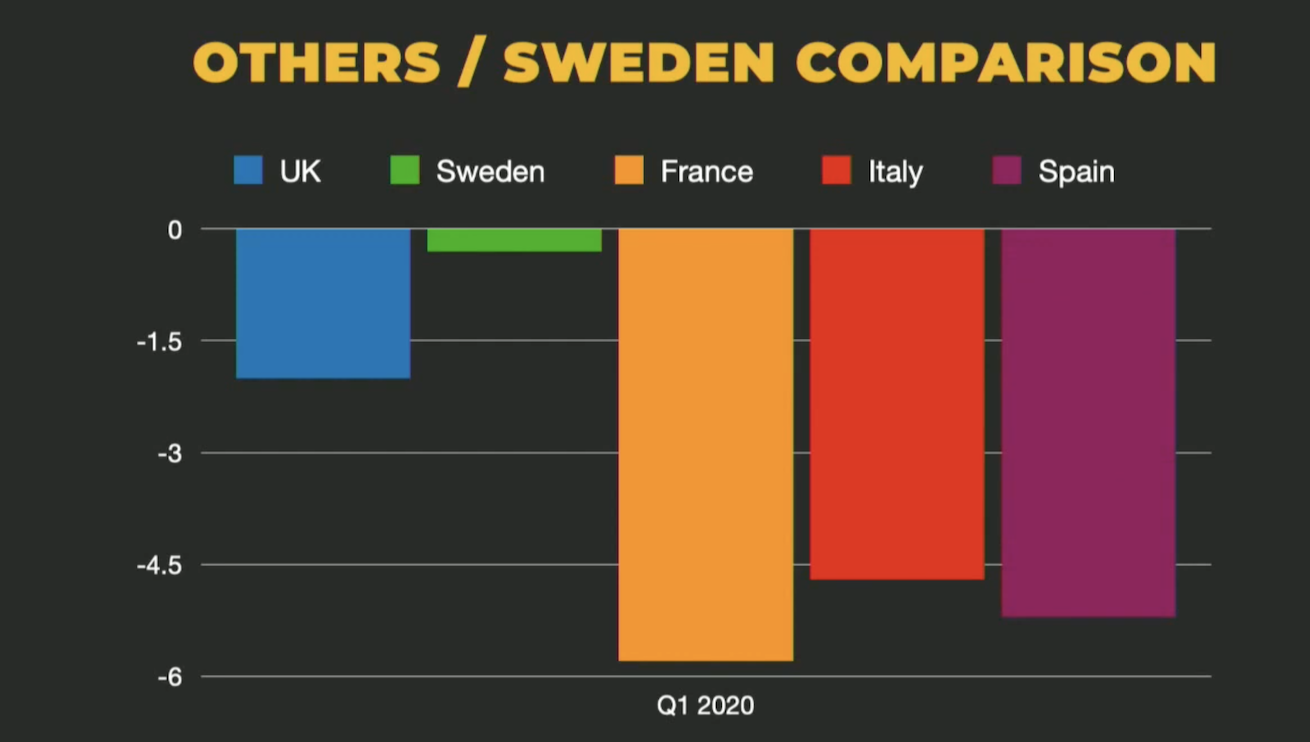
Sweden without a lockdown has not recorded more than 4500 deaths , which is less than the UK that suffered a rather stiff lockdown. The prime minister of Norway is on record saying that she had panicked initially and wished she had to some extent followed the Swedish model. The Swedes are probably close to some form of herd immunity with the icing of the least damaged economy in any European country. England faces a 14% drop in its GDP in 2020; such a recession was last seen in 1706.
Sweden kept its schools open. Children below 16 continued with school; bars and restaurants did not shutter down. The public was coaxed to follow simple common sense rules of social distancing, washing hands, and good hygiene. The Swedish public rose upto to the occasion. The government however made one big error, it failed to protect the elderly staying in care homes. The death count would have been considerably less had the government secured the elderly.
Almost half of deaths in other European countries are to be blamed again on the negligence regarding old folks in care homes.
It is also being realised that 30-40% excess deaths have been collateral damage. These are deaths not associated to Covid-19 but to people not seeking attention on time. A significant amount of deaths have been due to heart attacks at home. A lot of people feared going to hospitals because of their belief they would catch the SARS-CoV-2 virus or because there was no means of transport. Procedures in Cath labs across the globe have dropped by at least 40%. A lot of people are suffering angina silently and are resigned to their fate.
The psychological toll on people is yet to be estimated, but damage surely has been done. Anxiety and depression is rife in people corralled in their homes for months. Near absence of exercise, anxiety and mental stress must be accelerating plaque or blockage formation in coronary arteries. Minor strokes may be being ignored.
The second killer is cancer. The commonest are breast, lung, prostate and colon. Not necessarily in that order. Hundreds of people must be unaware that cancer in them has advanced to a more serious stage that may put their lives in peril. They however have not been able to get a consult and in many treatment has been postponed or denied altogether.
Who would have dreamt that the diminutive pill containing chloroquine would catch the attention of the entire world. Chloroquine was discovered in 1934 by a German scientist and became the drug of choice for treating malaria. I too took it when I was a third year student in medical college. I have never forgotten the dose since. Hydroxychloroquine (HCQ) , a sister drug, is currently used in auto immune disease such as lupus and rheumatoid arthritis. HCQ is able to quell immunity that attacks its own body in these 2 diseases. Donald Trump touted HCQ as a “game changer” in March. The result was a surge of 2000% in the prescription. Most doctors in the world were soon swallowing HCQ as a means of prophylaxis, that is as prevention from Covid-19. The ICMR issued an advisory on HCQ for post exposure prophylaxis without citing a single study. This was amazing stuff, far far away from evidence based science as we know it.
Observational studies published in leading journals did to show any clinical advantage with chloroquine or HCQ. These trials included a sizeable number of patients. A Spanish trial that included 700 patients of rheumatoid or lupus failed to show the slightest difference in those patients receiving HCQ or those not given the pill.
A Korean trial similarly failed to demonstrate efficacy of HCQ in an observational study of 300 people exposed to a confirmed patient of Covid-19.
Two papers from the US with more than a thousand patients did not demonstrate advantage with HCQ.
The largest observational paper that included 96000 patients form 671 hospitals across 6 continents also did not shown any improvement with HCQ, but suggested there may be harm. This paper is now being challenged for providing dodgy data. The editor of the Lancet has commissioned a third party audit to confirm the results. France has banned HCQ whilst Italy and Spain recommend use only in a clinical trial or in hospital setting.
The WHO had suspended the HCQ arm in the ongoing SOLIDARITY trial but has resumed it since yesterday. The New York Times and other leading newspapers of the world carry stories on the Lancet paper. Whether this will it be a storm in the teacup remains to be seen ?
Currently at least 200 ongoing trials on HCQ in patients with Covid-19. The results are awaited. Quite a few should be randomised. International trials are ongoing in the UK, France , the US and at the WHO. Results are eagerly expected in a few weeks or few months.
661
The new corona virus has taken a toll on the reputation of the authors of the big paper published in the Lancet. An independent audit has exposed flaws in data collection. The first author Dr. Mandeep Mehra has been compelled to retract the paper.
“It is now clear to me that in my hope to contribute to this research during a time of great need, I did not do enough to ensure that the data source was appropriate for this use,” Dr. Mandeep Mehra, lead author of the two studies, said in a statement to The New York Times.
“We can no longer vouch for the veracity of the primary data sources,” Mandeep Mehra of Brigham and Women’s Hospital, Frank Ruschitzka of University Hospital Zurich, and Amit Patel of University of Utah said in a statement issued by the Lancet. “Due to this unfortunate development, the authors request that the paper be retracted.”
Meanwhile, on Wednesday, researchers reported results of the first gold-standard clinical trial of hydroxycholoroquine in Covid-19, concluding that it did not prevent infections any better than placebo. This was published in the NEJM.
So far only 2 double blind randomised trials have been published. A Brazilian study published in JAMA showed that high dose chloroquine was as effective a slow dose chloroquine but lethality was much greater with the higher dose. The authors of the paper instead of appreciation faced death threats. The son of the Brazilian president with 2 million Twitter followers termed the study fake and the handiwork of the opposition political party. The principal author was compelled to go underground.
DOI: 10.1056/NEJMoa2016638
Yesterday the second double blind study on post exposure prophylaxis in 800 exposed people was published in the New England Journal of Medicine. The conclusion was that HCQ did not provide any benefit in preventing infection. Both groups ( HCQ and control ) developed Covid -19 to the same extent ; only 2 patients needed hospitalisation , one from each group, no patient died. The researchers concede that the population studied was 40 years and not all patients were confirmed by the RT-PCR test.
The new study included 821 people from across the United States and parts of Canada who had a either a high-risk or moderate-risk exposure to a person who had tested positive and was ill from the coronavirus. None of the participants had symptoms themselves. High-risk exposure meant they were less than six feet from a patient for more than ten minutes, with neither a mask nor a face shield. Moderate risk meant they wore a mask, but no face shield.
There was no meaningful difference between the placebo group and those who took the drug. Among those taking hydroxychloroquine, 49 of 414, or 11.8 percent, became ill. In the placebo group, 58 or 407, or 14.3 percent, became ill. Analyzed statistically, the difference between those rates was not significant.
The jury is still out on HCQ. We have to wait for more randomised trials to fill this huge gap. HCQ is cheap and made in the tons in India. It has shown activity against the virus in experimental conditions. But the chasm from the petri dish to the human body can be massive. The signal so far is that HCQ may not be the “game changer.”
India has recorded 6200 deaths over 6 months , at 4 per million population.
The “intellectuals” however had anticipated 20 lakh ( 2 million) deaths .
Extraordinary prescience , or covert agenda !
COVID-19 AND IMMUNITY IN SIMPLE LANGUAGE
A simple description of immunity in the body.
Sweden’s approach to Covid-19 does not appear to be the wrong move.
https://youtu.be/8lkb_NWjbbM
COVID 19 IN HINDI
The lockdown is being lifted. It is imperative that we do not permit fearmongers to operate amongst us. We should get back to normalcy employing common sense precautions.
DO NOT BE SCARED OF THE COVID-19 VIRUS
https://youtu.be/bZzyOMFwBW8
Is it Time to Rethink the Nationwide Lockdown Because of its Impact on the Most Vulnerable and Poor?
TREAT COVID-19 EARLY FOR BEST RESULTS
![]()
Data on mortality is coming in fast and furious. It is more our less clear that the mortality figure of 3.4% by the WHO was highly exaggerated. As was the 0.9 to 1% by the Imperial College, London. The infection fatality rate (IFR)is ranging from 0.2 to 0.4% across the globe. The Iranians have provided a figure off 0.12% , while the Germans have noted an IFR of 0.36%. Stanford University too reports 0.17% fatality while the University of Southern California suggests 0.2%. The mortality in India per million is one of the lowest in the world at 3 per million. The total number of cases so far are 139049 with 4024 deaths, giving a crude mortality of 2.89%. The number of infections should be at least 10 times more , hence the Indian infection fatality rate will be around 0.28 % to 0.028%; this is more or less akin to the mortality figures form other nations.
The deaths per million are strikingly less in Asian countries than Europe, China is 3, Bangladesh is 1, Pakistan is 5, Singapore is 4, Indonesia has 5, Japan is 5, South Korea is 5, and Malaysia is at 4 per million. The substantial difference in mortality can only be speculated upon, maybe younger population groups or higher local temperatures.
One should not worry too much on the increase in new number of cases in India. The prevalence is still reassuringly low, and even if there is a surge in new cases , we inch towards “herd Immunity.” I would prefer to term it “public” or “people” or even “community immunity” rather than herd immunity because the word “herd” is associated more with animals. A herd of elephants.deer, cows, horses, or sheep. We are people and not sheeple. A group of humans is better termed a clan of humans. I would not mind “clan immunity.”
The testing has been ramped up, so there is a bigger number of new cases each day. But a new case means an infection , not a death warrant. The majority of people will be asymptomatic or mildly symptomatic. Most of the patients landing up in hospital will be treated by oxygen alone. Till some time back 5-6% required intensive care management with high mobility and mortality. But with greater knowledge of the virus and treatment protocols this should be considerably lowered. We know that SARS-CoV-2 peaks very soon after symptom onset. Unlike SARS and MERS, in which the viral load peaks after a week, Covid -19 is characterised by the viral load at its highest within a week of symptom onset. The common flu is also accompanied by an early peak of viral load. The trick therefore will be to use an antiviral as soon as possible after onset of symptoms in patient with Covid-19.

DOI: 10.1056/NEJMoa2007764
A large double blind randomised trial including almost 1100 patients with CVovid-19 has reported significantly shortened recovery time with remdesivir as compared to placebo, from 15 to 11 days. There was also a rent towards lower mortality with remdesivir. Remedesivir acts against the enzyme polymerase that is essential for the replication of the Covid-19 virus. Interestingly remdesivir did not work in hepatitis nor was it very successful against ebola. Remdesivir, however, is currently considered the most promising therapeutic drug against Covid-19. There are other on going randomised trials with remdesivir and results are awaited. It is hoped that good sense prevails with the company manufacturing remdesivir; it keeps the price within reach of the common man. Bangladesh has already begun manufacturing the medicine by virtue of a special arrangement with Gilead, there should be similar understanding with Indian companies. Remdesivir was unable to reduce mortality below 5% (it did bring it down to 7%) in the trial, but this may have been because almost 25% patients were hooked to ventilators. Remdesivir was probably given too late in them. Patients reach the stage of ventilator support after the viral load has begun to diminish but the body has unleashed a wayward immunity response against itself, this is called the cytokine storm. The immune system attacks the lungs and other organs in the patients body with a vengeance. The antiviral now becomes incapable of treating the pathology.
Gilead Sciences has signed non-exclusive, licensing agreement with five generic manufacturers to expand access to its experimental antiviral drug remdesivir for Covid-19 patients.
The licensees include Mylan, Cipla, Hetero Labs and Jubilant Life Sciences in India, as well as Ferozsons Laboratories in Pakistan. The companies will be able to manufacture and distribute remdesivir in 127 countries.
However, a senior scientist at the Indian Council of Medical Research (ICMR) has said that “it will consider using the drug if Indian firms are able to make it,” as per the BBC. The ICMR continues with its antics.
May 8, 2020 https://doi.org/10.1016/ S0140-6736(20)31042-4
The other interesting randomised trial has emerged from Hong Kong. The researchers successfully cut down recovery time to 7 days alone with the use of a triple therapy combination. The troika consisted of lopinavir/ ritonavir (anti HIV), ribavarin (anti hepatitis C) and interferon versus lopinovir/ritonavir alone. The time to become negative for virus was only 7 days in the triple combination group as opposed to 12 days in the control group. Symptoms were alleviated in 4 days and there was suppression of interleukin levels. Raised interleukin levels indicate a grossly inflammatory state within the body. Treatment was given within 7 days from symptom onset. The researchers concluded that treatment with interferon should be initiated as soon a possible, definitely within a week of becoming ill. Interferon is considered the backbone of the triple combination treatment. The researchers have earlier shown reduction in mortality with the triple combination in patients with SARS. In the Covid-19 study, patients given triple therapy tested negative in 7 days as compared to 12 days in controls. Symptom duration was reduced from 8 to 4 days. The triple therapy worked when used early and probably will not give equally good results in patients on ventilators.

Two studies, one from Germany and the other from Singapore have confirmed that infective viral shedding is upto 10 days only. A patient may shed virus or be positive for as long as 6 weeks but will not be infective. After 10 days the PCR test is picking up dead virus. Till 10 days subgenomic messenger RNA can be seen in the Covid-19 virus, indicating that the virus can be isolated, cultured and above all is infective. If the virus ceases to be infective after 10 days , the protocol of 2 consecutive negative PCR tests becomes redundant. The viral load may be high after 10 days but the virus is not infective. Despite virus detection by PCR, the virus is not viable after 10 days. The PCR may detect high viral loads but the person concerned is not infective after 10 days of symptom onset.
The PCR test is best described by the inventor himself. Kary Mullis writes in his autobiography “Dancing naked in the minefield” that he figured out the PCR test one night as he drove back to his home with his future wife. He gives a nice analogy. Picking up a number plate of a car from the moon would be next to impossible. But this could be made easier if somehow the number plate was multiplied millions or billions of times. The human DNA is like a very long number plate. The SARS-CoV-2 has a genome or telephone number of 30000 numbers. Mullis imagined that a fragment of the DNA could be split into 2 by an enzyme, “polymerase.” The two fragments could again be split into two and then again into two; the reaction could go on. After 10 cycles we would have a thousand fragments , after 20 cycles a million and after 30 cycles a billion. It would become easier to identify the target fragment after this magnitude of amplification. Mullis called it the “polymerase chain reaction” and soon the PCR test came into being. It could not only be helpful in solving crimes but could also be used to study the DNA of an animal that existed 40,000 years ago. The PCR test is used to detect the presence of the Covid-19 virus. The test is not infallible because errors in collection of sample and transportation can account for a negative test. But more about the fact that the PCR test can be quite fallible some time later.
The take home message is that combination antiviral treatment is a must in Covid-19, and this should be begun within a week of symptom onset. But selection of the patient who would most benefit from treatment remains unclear.
HYDROXYCHLOROQUINE PROPHYLAXIX FOR COVID-19
India has one of the lowest death rate at 3 per million population; there is as of now no evidence that hydroxychloroquine is effective for prophylaxis; the ICMR provides no reference in its advisory ; vaccines are being tested at “warp speed”; lets hope one works.
The QT interval in patients with COVID-19 treated with hydroxychloroquine and azithromycin
Nature Medicine (2020)
JAMA | OriginalInvestigation
Association of Treatment With Hydroxychloroquine or Azithromycin With In-Hospital Mortality in Patients With COVID-19 in New York State
Eli S. Rosenberg, PhD; Elizabeth M. Dufort, MD; Tomoko Udo, PhD; Larissa A. Wilberschied, MS;
Jessica Kumar, DO; James Tesoriero, PhD; Patti Weinberg, PA; James Kirkwood, MPH; Alison Muse, MPH; Jack DeHovitz, MD; Debra S. Blog, MD; Brad Hutton, MPH; David R. Holtgrave, PhD; Howard A. Zucker, MD
JAMA. doi:10.1001/jama.2020.8630 Published online May 11, 2020.
Hydroxychloroquine Versus COVID-19:
A Rapid Systematic Review and Meta-Analysis
Amir Shamshirian1,2, Amirhossein Hessami3, Keyvan Heydari2,3, Reza Alizadeh-Navaei2, Mohammad Ali Ebrahimzadeh4, Roya Ghasemian5, Elham Aboufazeli6, Hananeh Baradaran7, Keyvan Karimifar8, Aida Eftekhari8, Danial Shamshirian9*
The new england journal of medicine Original Article
Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19
This article was published on May 7, 2020, at NEJM.org.
DOI: 10.1056/NEJMoa2012410