
Continue reading “PHOTOS TAKEN BY MY DAD , MR. K.NATARAJAN , MA.”
Continue reading “PHOTOS TAKEN BY MY DAD , MR. K.NATARAJAN , MA.”
The Future Revascularization Evaluation in Patients with Diabetes Mellitus :Optimal Management of Multivessel Disease (FREEDOM) was the largest randomized trial studying the impact of percutaneous intervention (PCI) with drug eluting stents (DES) versus CABG in patients of diabetes mellitus with multivessel disease. Nineteen hundred diabetic patients (mean age 63 years) were enrolled in 140 international centers; 83% had 3-vessel disease and 71% were men. The DES group received sirolimus or paclitaxel eluting stents, which are now considered first generation DES. Median follow up was 3.8 years. The primary outcome (death from any cause, nonfatal myocardial infarction (MI) or nonfatal stroke) was significantly more common in the PCI patients (27% vs. 19%; p=0.005); driven largely by rates of myocardial infarction (p<0.001) and death from any cause (p=0.049). The CABG group had both lower mortality (6% vs. 13%) and MI (11% vs.16%). Strokes were however more common with CABG (5.2% vs.2.4%; p=0.03). The authors concluded that CABG was superior to PCI in diabetic patients in that it significantly reduced death and MI (1).
Continue reading “FREEDOM FOR PCI IN DIABETIC PATIENTS WITH MULTIVESSEL CORONARY ARTERY DISEASE.”
Percutaneous intervention (PCI) has become standard care for treatment of patients suffering from acute coronary syndrome consisting of ST-elevation myocardial infarction (STEMI), non ST-segment elevation myocardial infarction (NSTEMI) and unstable angina. The procedure demands, for success, adjunctive therapy in the form of antiplatelet agents and anticoagulants. The Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) trial established the role bivalirudin (a direct thrombin inhibitor); the trial compared bivalirudin with heparin plus a glycoprotein inhibitor (GPI) in patients with STEMI, with bivalirudin recording survival benefit extending to 3 years, albeit with a 5 fold increased incidence of stent thrombosis (ST) (1).
Continue reading “HEPARIN IS MORE THAN A MATCH FOR BIVALIRUDIN.”
This week JAMA Internal Medicine published a massive retrospective study that included almost a million subjects. Almost half a million people taking statins were compared to an equivalent population not popping any. They also added more than 26,000 patients on non-statin lipid lowering drugs. The authors observed, in their own words, a strong association between first exposure to statins and acute memory loss diagnosed within 30 days following exposure. The increase in memory loss was 4.40 times compared with non-statin users; in other words statins hiked up loss of memory by 440%.


A recent New York Times article on the toxicity of Delhi’s air not only set the cat among the pigeons but compelled the Hindustan Times (a daily) to print a series of reports on it’s front page emphasizing the same. The Times quotes a remarkable study commissioned by Central Pollution Control Board; which then sat over the conclusions drawn by the investigators for more than half a decade. The study assessing lung functions in almost 6,000 Delhi school children from 36 schools (begun in 2002) found that 44% suffered from poor or restrictive lungs, and that 10-27% of them complained of headache, eye irritation, nausea, palpitation and fatigue. The Times correspondent decided enough was enough when he found that his little boy had developed full blown severe asthma necessitating hospitalization.



The last quarter of the eighteenth century substantially altered the complexion of the planet; the Yanks prevailed over the Brits under George Washington in the Battle of Princeton and the subsequent birth of the most powerful nation on Earth (January 1777). The Brits, however, 2 decades earlier had overcome Siraj-ud-Daulah in the Battle of Palashi (Plassey) to herald British imperialism over the Indian subcontinent,(courtesy the treachery of Mir JAfar). It istill unclear whether Robert Clive bribed Mir Jafar to betray the Nawab of Bengal or Mir Jafar enticed Clive with a pay off to attack the Nawab with the assurance of deception in the heat of battle; anyway this classic non-military maneuver would be employed repeatedly by the English as they overran an ancient but corrupt civilization. The historic betrayal by Mir Jafar (not the first or last by an Indian) took place in June 1757.
Transcatheter aortic valve replacement (TAVR) has rapidly emerged as a viable alternative for the treatment of severe symptomatic valvular aortic stenosis (AS). Almost 100,000 patients of AS have benefited from this technique. Symptomatic severe AS is a killer that needs prompt surgical intervention. The PARTNER trials established the superiority of TAVR over medical management in inoperable cases, and equivalence with surgical valve replacement in high-risk patients of AS. The UK Registry of 870 patients with mean age of 82 years now provides long- term data on efficacy of TAVR from 25 centers spread out in England and Wales.
Continue reading “TAVR FROM THE FIRST CASE IN 2002 TO THE UK REGISTRY IN 2015.”


The revenue department of the government of Maharashtra revealed that 422 farmers had killed themselves by the first week of December 2014. There were 77 suicides in Beed, the home district of former union minister Gopinath Munde, 44 in Nanded which is the former home district of former chief minister Ashok Chavan and 18 suicides took place in Latur, the home district of another former chief minister Vilasrao Deshmukh. The farmers were culling themselves because they were simply unable to cope with debts accrued and crop losses due to sparse irrigation and mitigating rain fall. The Vidarbha Janandolan Samiti (VJS) an NGO following farmer suicides recorded 1022 deaths in the cotton belt of Maharashtra alone. Mercifully the current chief minister has acknowledged these suicides and promised to garner a Rs. 4,500 crore (Rs. 450 million) financial package from the federal government.

The RIVAL study had randomized 7021 patients of acute coronary syndrome (mean age 62 years; 14% more than 75; 28% ST-segment elevation myocardial infarction-STEMI) to either radial or femoral access for coronary angiography and planned PCI between 2006 and 2010. It was seen that at the end of 30 days, the rate of the primary outcome (a composite of death, myocardial infarction, stroke and major bleeding unrelated to coronary artery bypass graft surgery) was the same in both groups. Large hematomas and pseudo aneurysms needing closure occurred significantly less in the radial group than in the femoral cohort (1.2% vs. 3.0% and 0.2% vs. 0.7% respectively). Cross over rates from radial to femoral approach due to vessel spasm or tortuosity was greater than femoral to radial (7% vs. 0.9%) and fluoroscopy was significantly longer in the radial than in the femoral group (9.8 vs. 8 minutes, p< 0.001). It was concluded that albeit both approaches had similar clinical outcomes the radial approach resulted in less local complications, less bleeding and earlier ambulation. The RIVAL data was published in 2011.
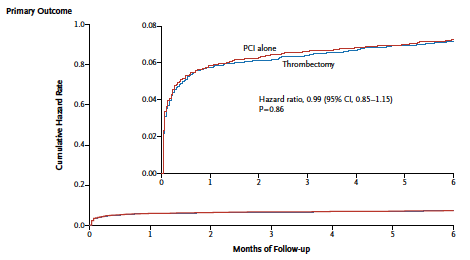
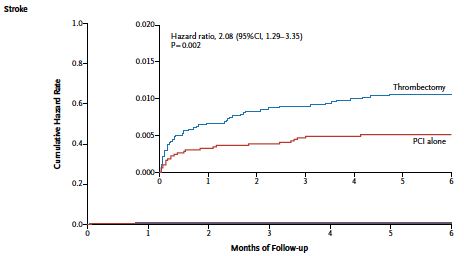
The final nail in the coffin of manual thrombo-suction (MT) during treatment of acute STEMI has been delivered in this week’s ‘TOTAL” trial published in the NEJM. The TAPAS study had in randomized manner shown reduced mortality with MT some years ago in a cohort of more than 1000 patients of STEMI followed for a year. Manual thrombo-suction was considered effective and safe and therefore widely practiced during primary PCI. The procedure was simple, inexpensive and intuitively appeared to produce excellent results. TAPAS (a single center study) was however underpowered for hard clinical endpoints and their results were reckoned hypothesis generating.
Continue reading “THE ‘TOTAL’ REQUIEM FOR MANUAL THROMBO-SUCTION IN PATIENTS WITH STEMI.”
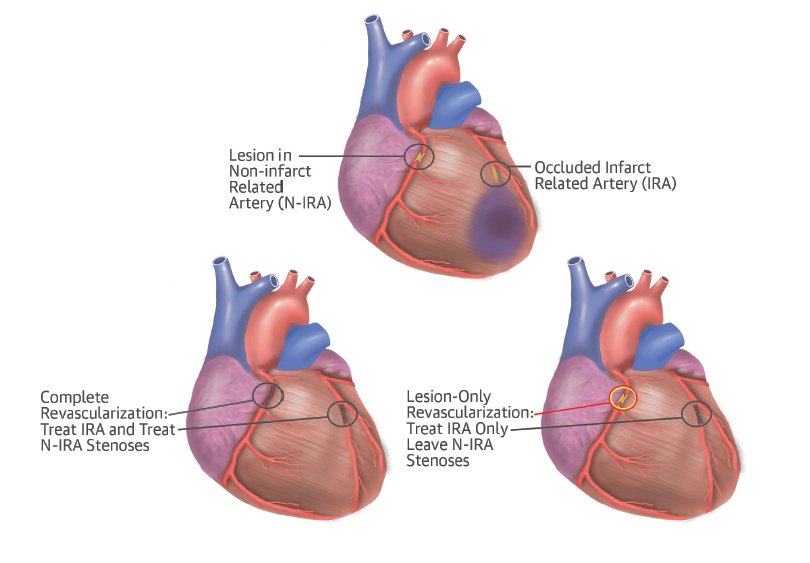
Primary percutaneous coronary intervention (PPCI) is the established technique for restoring flow in the infarction related blocked artery (IRA) in the setting of acute ST -segment elevation myocardial infarction (STEMI). Numerous randomized studies have confirmed that PPCI significantly reduced mortality, re-infarction and stroke as compared to thrombolytic treatment. What is however still not clear is what is to be done with the other coronary arteries if found blocked during PPCI; bearing in mind that approximately 30% to 40% of patients undergoing primary PCI for acute MI have multi but meta-analysis and observational studies have shown mixed results for complete revascularization. The guidelines had frowned upon tackling non-IRA in setting of STEMI and most physicians are reluctant to stent non-IRA because of the fear of complications and prolongation of the procedure. All professional cardiac societies recommend treating non-IRA only if hemodynamic compromise persists after opening up the IRA.
The Journal of American College of Cardiology shall publish the 5 years follow up of the PRECOMBAT (Premier of Randomized Comparison of Bypass Surgery versus Angioplasty using Sirolimus Stents in Patients With Left Main Coronary Artery Disease) trial data presented in the recent American College of Cardiology 2015 Scientific Sessions. The PRECOMBAT trial randomized 600 patients with unprotected left main artery stenosis in 13 Korean sites to PCI with a sirolimus eluting stent (SES) or CABG (300); these patients had angina, non ST-segment elevation myocardial infarction or silent ischemia. Their mean age was 62 years, one third had diabetes and half had unstable angina. The SYNTAX score was about 25 in both groups. More than 70% had left main with 2 or 3 vessel disease.
Continue reading “‘PRECOMBAT’ OR ‘SYNTAX’ FOR LEFT MAIN DISEASE.”
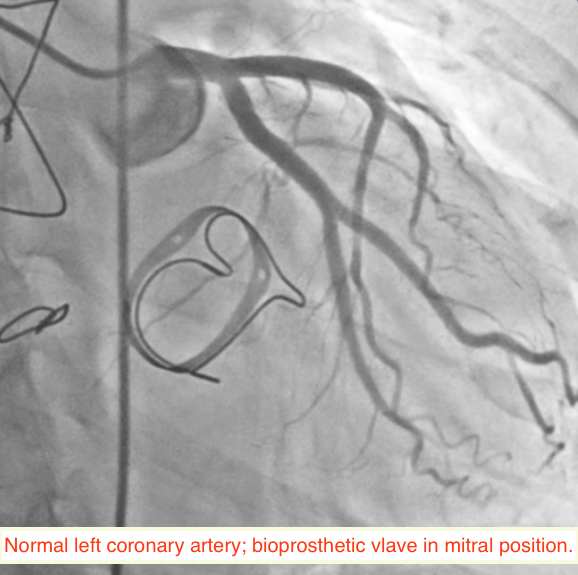
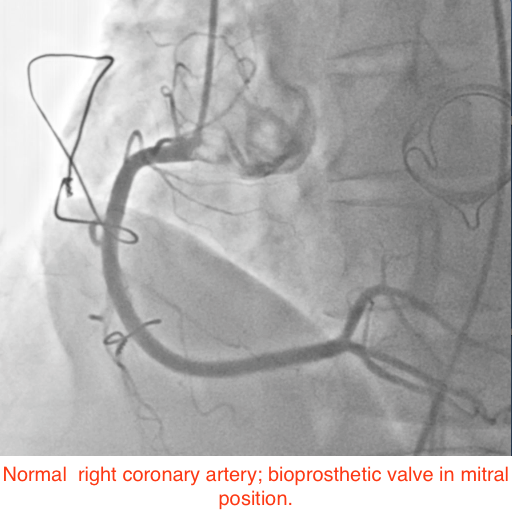
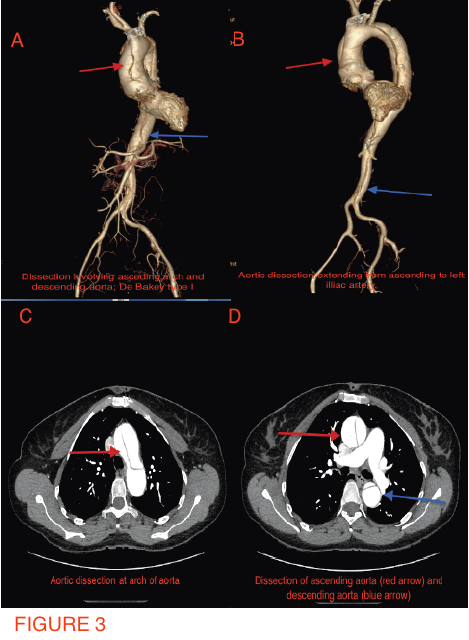
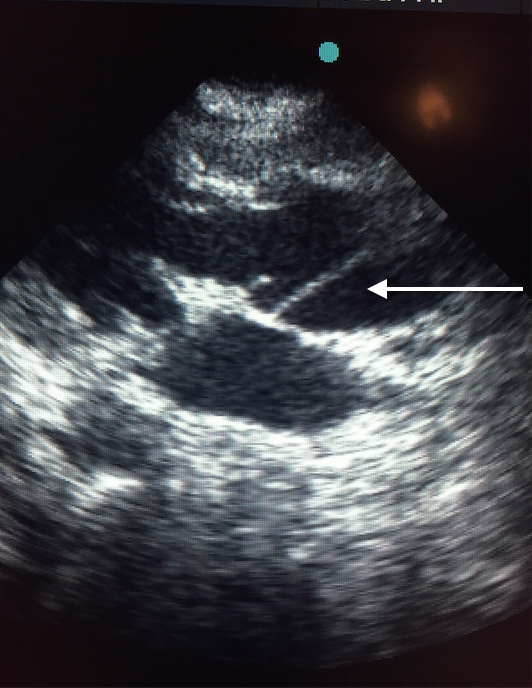
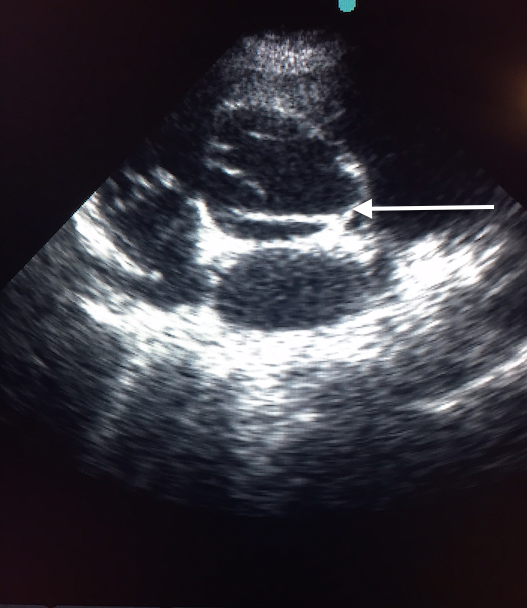
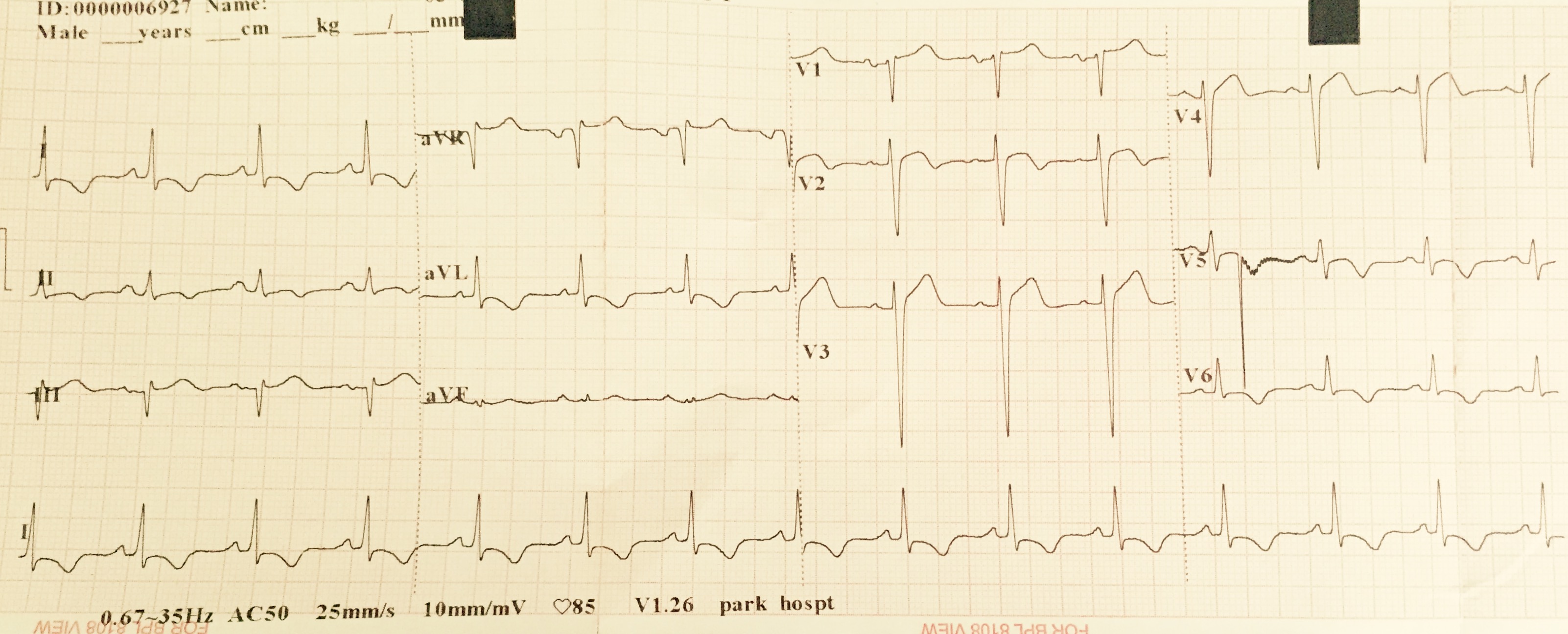
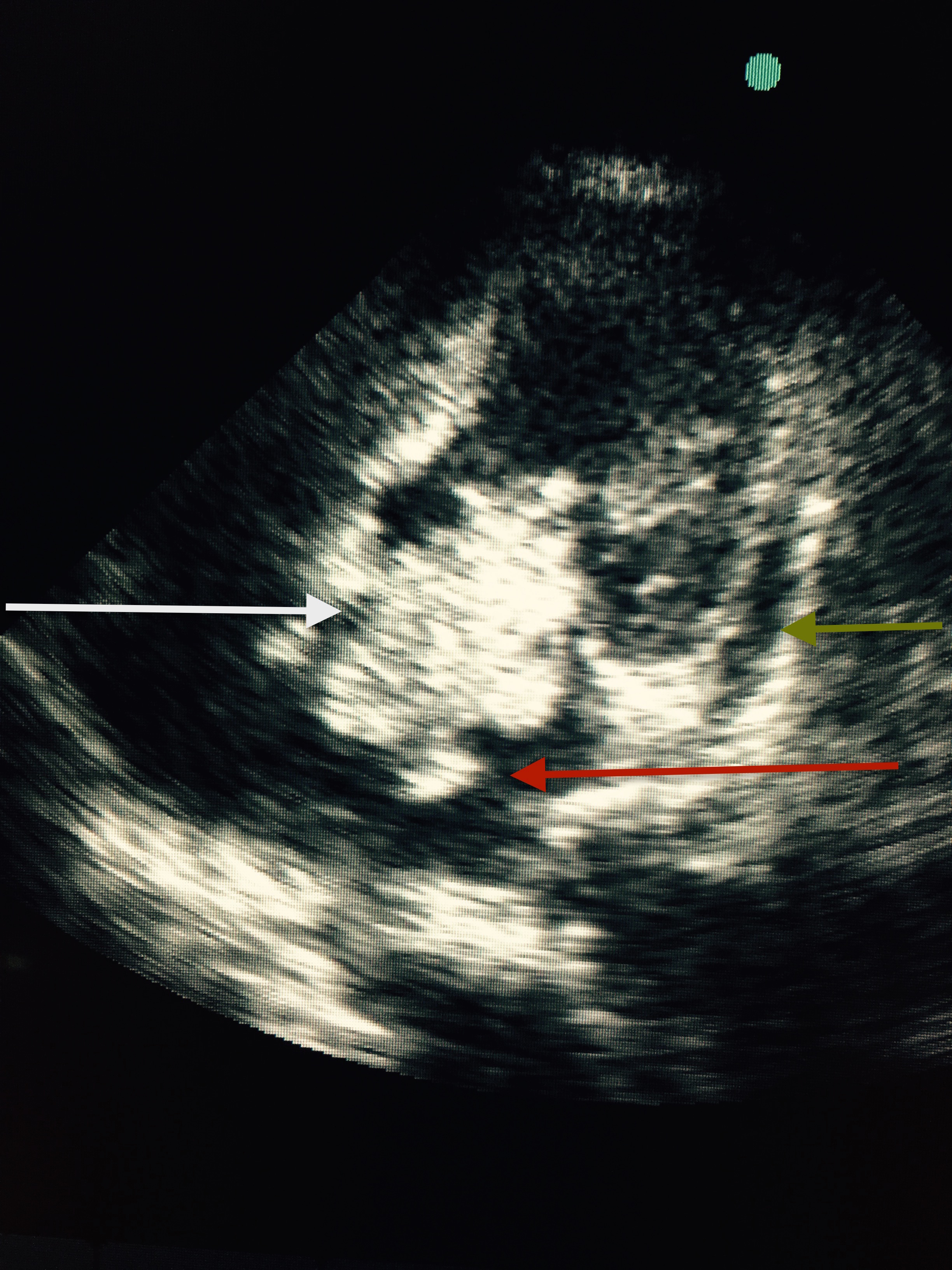
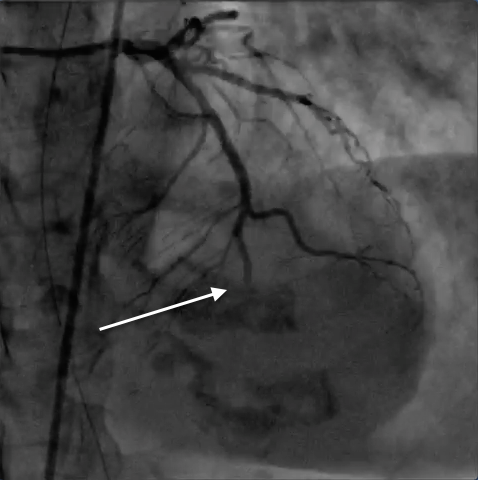
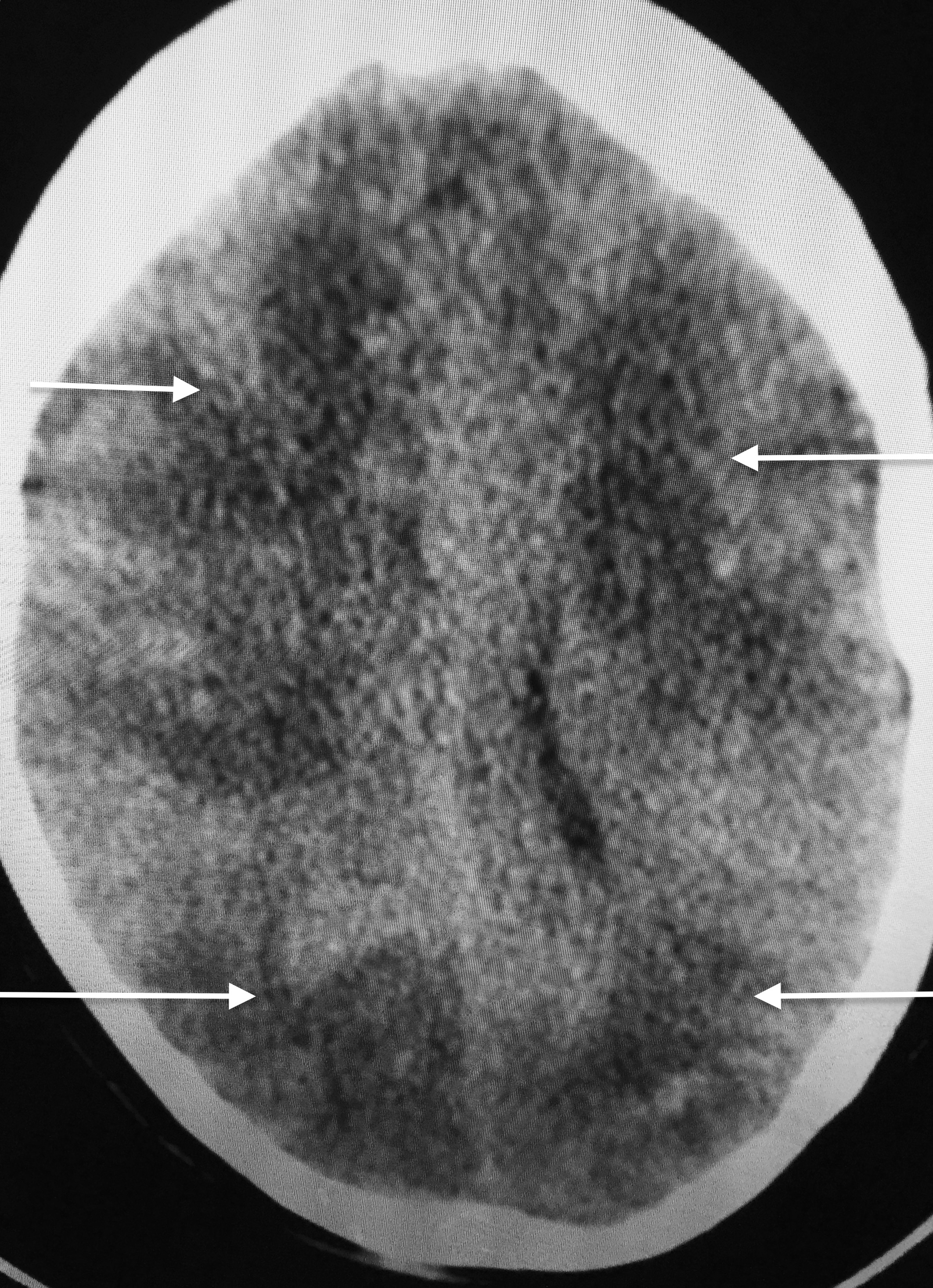
A 49-year-old woman suffering from hypertension for the past 5 years, and who had undergone mitral valve replacement with a bio-prosthetic valve a decade ago for rheumatic mitral regurgitation, was admitted for sudden onset severe tearing pain in her throat, followed by pain in the inter-scapular region, and then heaviness over the chest in an outside hospital 6 weeks ago. She was managed then with analgesics as the ECG displayed no changes and her cardiac biomarkers were normal. Invasive coronary angiography done during the current admission for intermittent pain in her left shoulder demonstrated normal coronary arteries (Figures 1-2). She underwent a multi-detector 256 slice computed tomography contrast aortography (CTA) that revealed extensive aortic dissection involving the ascending aorta (Figures 3A and 3B, red arrow), the arch (Figures 3A and 3C, red arrow) and descending aorta up to her left iliac artery (Figures 3A and 3B, red arrow, and Figure 3D, blue arrow); cross sectional CTA showed dissection of her ascending (Figure 3D, red arrow) and descending aorta (Fig 3D blue arrow). The aortic root and ascending aorta were dilated measuring 4.6 X 5.7 cm in AP dimensions. There was no sign of an intramural hematoma.
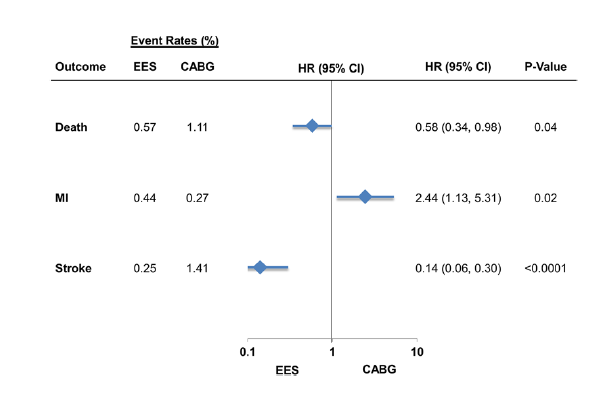
Physicians continue to agonize over decisions on the best treatment option for multi-vessel (MVD) coronary artery disease. We discuss over here not left main disease; which apparently is a different disease from multi-vessel disease in terms of clinical outcomes with percutaneous coronary intervention (PCI) as has been seen in 5 years follow up of the SYNTAX trial. We shall focus on 2 big trials presented in this year’s ACC Meeting and simultaneously published in the NEJM. Both studies (one randomized but underpowered and the other a large observational one) come up with conclusions that death rate was similar between CABG surgery and PCI in patients with MVD. The rates of spontaneous myocardial infarction and repeat revascularization were greater in the PCI groups then in patients who underwent CABG. Both trials used a second generation drug eluting stent (DES) that is well known (as seen in randomized trials) to result in significantly lesser death, myocardial infarction, restenosis and stent thrombosis than earlier generation DES and bare metal stents.
Continue reading “PCI OR CABG FOR MULTIVESSEL CORONARY ARTERY DISEASE ?”

High levels of low-density lipoprotein (LDL) cholesterol result in increased prevalence of coronary heart disease (CHD) such as myocardial infarction, stroke, unstable angina requiring hospitalization , heart failure and death. In recent years, oral statin drugs have shown significant reduction in CHD clinical events in large randomized trials and meta-analyses. But does lowering of LDL levels by non-statin drugs also reduce clinical events? The answer has not been always in the affirmative. In fact 2 large randomized studies using the drug niacin failed to reduce clinical events despite considerable lowering of LDL cholesterol and increase in the “good cholesterol” (high-density lipoprotein: HDL); niacin actually caused serious adverse effects.
Continue reading “THE LATEST CHOLESTEROL BUSTER : PCSK9 INHIBITORS.”

Mr.Jinnah’s political and ideological narratives have not been assessed through the prism of his tuberculosis. Patrick French ( historian and biographer) is skeptical that Jinnah ever had tuberculosis, while other historians acknowledge the ailment, but in passing. French sticks to the diagnosis of bronchiectasis without providing any evidence except for notes of Pakistani historian ZH Zaidi. Largely most historians have considered Jinnah’s TB as an innocent bystander that did not in any way influence or compromise his thoughts and attitudes.
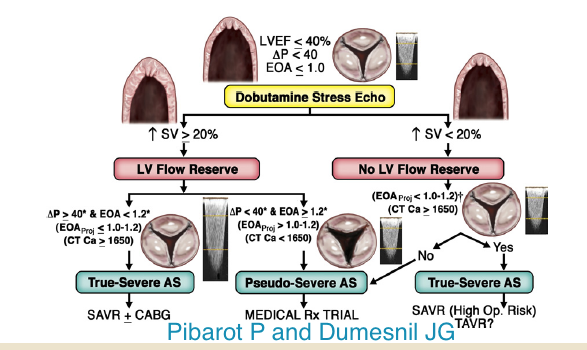
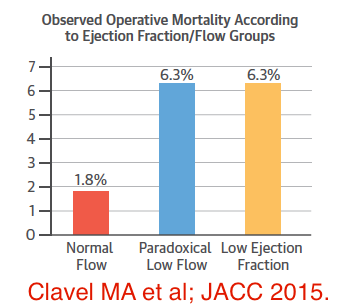
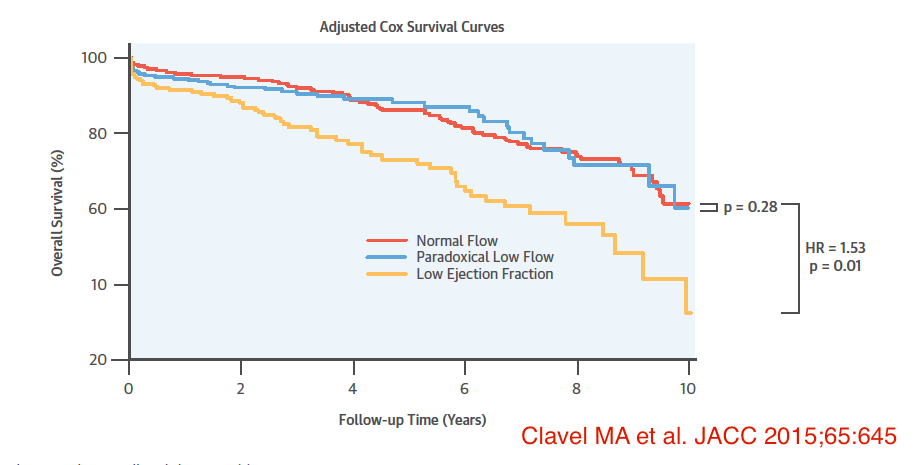
Low flow aortic stenosis (LF) with low left ventricle ejection fraction (LVEF) or normal LVEF continues to perplex physicians and cardiologists alike. The terms are confusing and the management strategies still are to be sorted out. An excellent Canadian paper describes clinical outcomes with aortic valve replacement (AVR) in these subsets of patients in the latest issue of JACC. But first we need to define these groups of patients. Severe valvular aortic stenosis (AS) is defined as aortic effective orifice area (EOA) of less than 1 cm2 or < 0.6 cm2/ m2 if indexed to body surface area, a peak echo velocity jet of more than 4 m/sec, and a mean gradient greater than 40 mm Hg. Surgical intervention is mandatory when a patient with severe AS becomes symptomatic with chest pain, breathlessness or syncope. Aortic valve replacement (AVR) is also recommended for asymptomatic patients with severe AS who would need CABG/ another valve surgery, poor LVEF (< 50%), or a patient who gets symptoms while doing an exercise ECG (TMT) test.
Continue reading “THE DILEMMA OF “LOW FLOW-LOW GRADIENT” AORTIC STENOSIS”
No new drug for systolic heart failure (HF) has been approved by the FDA for more than a decade; the last one being eplerenone (an aldosterone antagonist) which was approved in 2003. In 2005 a combination drug of hydralazine –isosorbide dinitrate was cleared for (HF) for African Americans who persisted with symptoms despite evidence based treatment. Finally after so many years of research a new combination tablet has made head lines across the globe for significant reduction in mortality in HF patients already on standard treatment including 10 mg twice a day of enalapril. The novel drug has been given the rather mundane name of LCZ696, and consists of a combination of a neprilysin inhibitor (sacubitril) and the angiotensin receptor blocker (ARB) valsartan (160 mg).
Continue reading “A PARADIGM SHIFT IN CONGESTIVE HEART FAILURE THERAPY.”


The recently concluded European Society of Cardiology 2014 Conference (one of the largest cardiology meetings in the world) in Barcelona, Spain was dazzled by a striking study that showed dramatic efficacy of an experimental drug in patients with heart failure. The new drug, with the tonguetwisting name of ‘LCZ696’, reduced both deaths due to cardiovascular disease and hospitalization due to heart failure in patients already prescribed standard life saving medication by a whopping 20%. This study (PARADIGMHF) included more than 8000 heart failure patients (1). Heart failure affects more than 26 million (260 lakh) people globally and is the leading cause of hospitalization in Europe and the US. A patient with heart failure is unable to pump blood adequately to different organs of the body, because of a weakened heart due to a variety of reasons such as heart attack and hypertension. This leads to breathlessness, tiredness, salt retention, and swollen feet and eventually, if not treated, death. The new drug has therefore created a buzz among physicians across the world; but it will cost around $ 2,500 annually as opposed to $ 50 a year spent on available heart failure medicines. It will be therefore a multi-billion dollar bonanza for the drug company that has made the new drug ‘LCZ696’. Fiscal profit, albeit justifiable, is the driving force behind pharmaceutical research for new drugs. There have been hundreds of rigorously controlled randomized trials on drugs and devices in cardiovascular disease; acute heart attack in fact is not only the most extensively studied disease in the world but has also turned into a multi billion dollar industry. There is, however, sparse randomized data on the role of diet in prevention of heart attack and stroke. The public is repeatedly bombarded with anecdotal or observational nutritional information on prevention of cardiovascular disease.