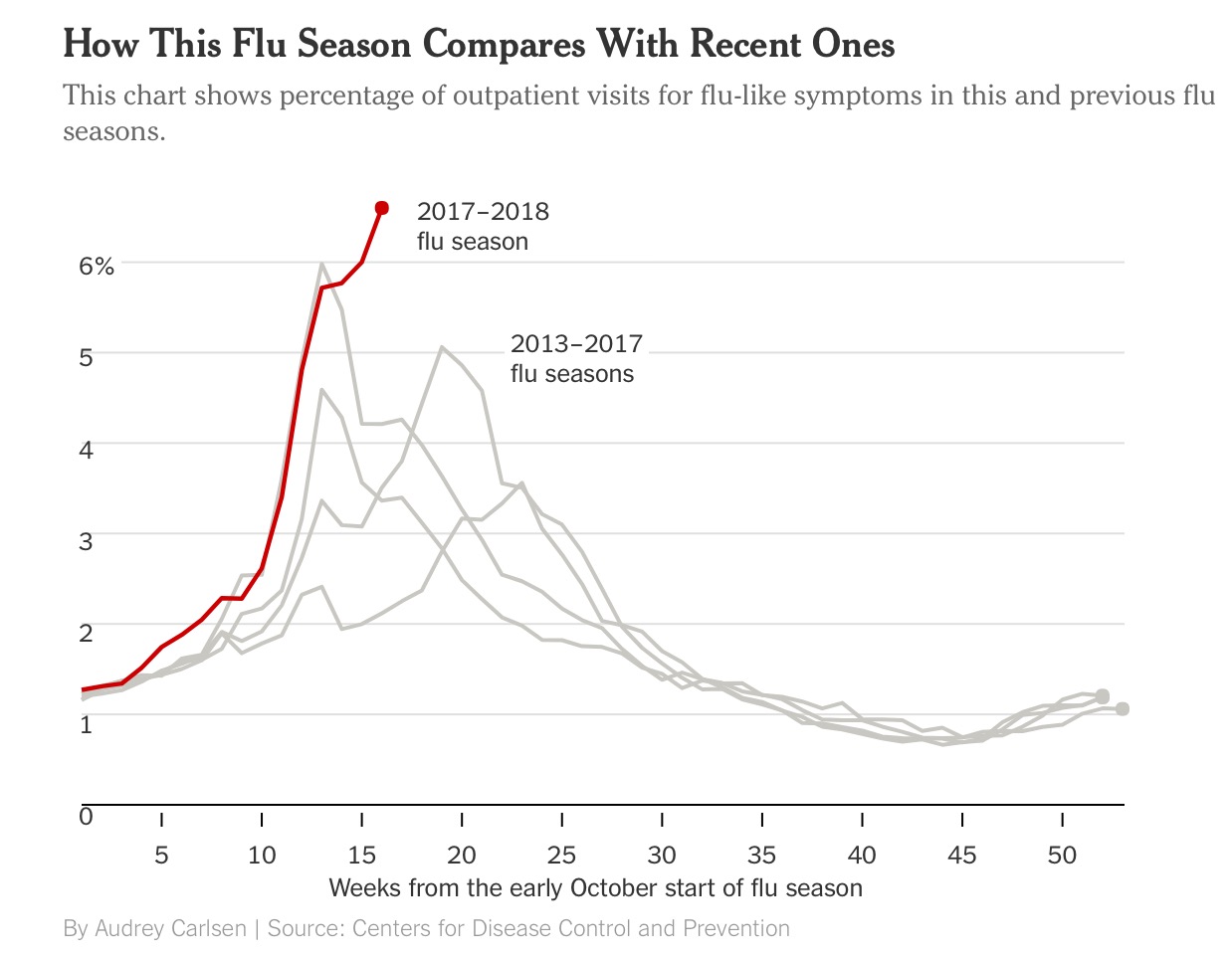
As the flu epidemic tightens its grip both in the U.K. and the US it is abundantly clear to scientists that the predominant culprit is the H3N2 subtype influenza A virus. The H3N2 virus subtype is disliked by physicians because it is far more potent than the other A and B influenza virus. H3N2 is capable of rapid transformation to elude the immune system of the human body. It is also associated with more severe symptoms, hospitalisation and death. The other troublesome fact is that vaccination against the H3N2 subtype is feeble, in fact influenza vaccination has been found to be effective for prevention in only 10% of people over 60 years. Vaccines against measles provide 97% protection and over 90% protection against small pox and polio. In short the flu vaccine is far from perfect. Currently more than 6% of people visiting outpatient departments of hospitals in the US are suffering from flu like symptoms, significantly greater numbers than previous years.
People with mild symptoms are best managed at home with lots of oral fluids and rest. In case symptoms are severe, or the elderly, or people with chronic disease such as diabetes, asthma, chronic heart disease, treatment may be initiated with Tamiflu within 2 days of symptom onset. Tamiflu does not reduce mortality but may reduce duration and severity of symptoms. Pregnant women with flu are considered high risk for complications. People down with flu are advised to wash hands frequently with soap, isolate tooth brushes and wash their bed sheets/pillow covers every third day. Recovery from flu usually takes 5-7 days. Antibacterial wipes should be used to wipe remotes, switches and door knobs. The British Medical Journal had warned that oseltamivir or tamiflu was no better than paracetamol in patients with flu, but research by the London school of hygiene and tropical medicine reported that tamiflu significantly cuts incidence of serious complications such as pneumonia. This report a meta analysis for whatever it was worth got published in the Lancet. Crucially tamiflu can cause nausea and vomiting, worse it has been reported that 8 Japanese children committed suicide after taking tamiflu.
Continue reading “CAN THE FLU VACCINE PREVENT A HEART ATTACK ?”