A micron is a millionth of a meter. A strand of human hair is approximately 50 microns wide while the red blood cell carrying oxygen in our blood is just 5 microns wide. One sneeze or cough may carry about 3,000 droplets, with each droplet being more than 5 microns across. When the suspended particle is smaller than 5 microns, it is called an aerosol.
Author: admin
Why Testing Is So Important for Tackling Coronavirus in India

You can be certain Prime Minister Narendra Modi is quite aware that tackling the COVID-19 pandemic will take more than one day of self-imposed quarantine by the people. Nonetheless, he deserves to be lauded for his efforts because, in all probability, he has sensitised the people of India for future lockdowns of longer duration, as the Chinese authorities imposed in Hubei province and as is increasingly being the case across Europe, including in Spain, France and Italy.
COVID-19 AND THE GUT
2020
Published Online
March 19, 2020 https://doi.org/10.1016/ S2468-1253(20)30083-2
First the unvarnished fact, without the slightest intention of grabbing brownie points. A scientific letter was published last week in the “Lancet Gastroenterol Hepatol Journal” that reported results of the presence of coronavirus in respiratory and faecal samples confirmed by real time reverse transcription polymerase chain reaction (RT-PCR). Respiratory and faecal samples could be collected from 74 of 98 patients infected with Covid-19 (76% of patient group). Respiratory swabs remained positive for 15.4 days from symptom onset. Faecal samples were positive in 41 (55%) of 74 patients and remained positive for 27.9 days, while the respiratory swabs remained positive for only 16.7 days after first symptom onset. Simply put patients infected with Covid -19 had virus in their stools by an average 11 days more than in their respiratory swabs . However,45% of patients had negative faecal samples, that is almost half of the patients did not have their guts infected with Covid-19. Some crucial observations pointed out by the researchers need to be emphasised; presence gastrointestinal symptoms was not associated with faecal viral positivity; severity of disease was not associated with extended duration of virus in faeces; but importantly there was an association of faecal virus with anti-viral treatment.
The authors of the letter suggest that routine stool sample testing should be done by RT-PCR even after respiratory samples become negative. But they concede that do not know whether the virus in stool is viable based upon RT-PCR testing; and that no case of transmission has been reported by the faecal-oral route with Covid-19 : “which might suggest that infection via this route is unlikely in quarantine facilities, in hospital, or while under self -isolation.” Further studies are obviously needed to to determine viability and infectivity of Covid-19 in faeces. Based upon this scientific letter the plausible conclusions we can draw are the Covid-19 virus is present for more days in faeces, but little is known of the viability and infectivity of this virus. Crucially the letter does NOT mention transmission of Covid-19 by flies anywhere.
The news report by Hindustan Times today quoting a famous Bollywood celebrity therefore comes a surprise. The Hindustan Times elaborates “If the house fly sits on this excreta and then on some food particles and spread the disease.” It is possible this is a hacked tweet. It certainly is not based on any scientific peer reviewed publication. Hindustan Times provides a reference but this is a comment on recommendations for stool transplant from prospective donors, who should be screened for typical Covid-19 symptoms within the previous month, travel to areas infected by Covid -19 or close contact with an infected person. If any of the above are present such a donor must have confirmation by RT-CRP testing. The recommendations would be applicable to all types of donors. Incidentally faecal microbiota transplantation is now successfully being used in the management of recurrent Clostridoides difficile infection.
The study cited by Hindustan Times is not on faecal-oral transmission of Covid-19 but does provide a reference of a study (yet to be proof read) on 73 patients infected with Covid-19 virus. Of the 73n patients about half were stool postive for a duration ranging from 1 day to 12 days. About 23% patients persisted with positive stool samples after respiratory samples had become negative. The authors note that their study provides evidence of gut infection and its “possible” faecal-oral route transmission. Entry into the gastrointestinal tract is by ACE 2 receptors present in the stomach, duodenum and rectum. The CDC recommendation that once a patient has 2 consecutive negative respiratory samples can be considered disease free may not hold because of extended presence of the virus in the gut. But again this paper too does not dare to make specific extrapolations on infectivity by this route.
The global pandemic has brought the planet to standstill. Economies across the world are getting brutally battered. Scientists are scrambling to provide answers. There have been mixed signals regarding the new disease in almost every country. Understandably people are under extremes stress; but it is exactly in such times that we have hold our nerves. It is imperative that we keep our wits about us and gather information from peer reviewed publications in scientific journals. Newspaper headlines albeit interesting could be quite misleading or worse add to the confusion. Never before has the lay public needed to pay more attention (only) to qualified scientists; this hold good for any country, but especially for us in India. Celebrities for all their laudable efforts in disseminating information may inadvertently add to the chaos. We cannot afford a Mr. Idris Elba staring into the camera in all seriousness to announce that he is infected with Covid -19 with his wife (Covid-19 negative) next to him. Obviously Mr. Elba, good enough to be in the James Bond loop for years, is completely unaware that he is sending the wrong message, or he is quite sure he will not transmit the virus to his wife. Silence was never more golden.
The Indian ministry of health has a website up with daily bulletins on the do’s and dont’s regarding the Covid-19 virus.
LOSS OF SMELL; NEW SYMPTOM OF THE COVID-19 DISEASE
The coronavirus juggernaut is exactly that, merciless and destructive. The pandemic just refuses to be tamed or slowed down. The social, economic and clinical complexities keep evolving by the day. Each new day brings incremental information on the new virus. Launched from Wuhan, it put the fear of God in northern Italy, and today the United States has become epicentre of the pandemic. Johns Hopkins University suggests that the United States has the world’s largest numbers (more than 82,000 of Covid-19 cases) with about 1200 deaths, giving a case fatality ratio of 1.5%. Globally there are more than 500,000 cases now. India has announced more than $ 23 billion economic stimulus plan for the millions of people affected by the largest lockdown in the world. Mercifully number of deaths so far are relatively less than other nations. Even as I write the UK prime minister Boris Johnson has tested positive for Covid-19. He has fever accompanied by persistent cough, and shall self isolate in Downing Street. In his own words: “I have developed mild symptoms of the coronavirus that is to say a temperature and a persistent cough…stay at home , protect the NHS and save lives.” Luckily for him he manages the short 2 minute video recorded message without a sniffle, sneeze, or a cough.
We know from Chinese data of 1099 confirmed patients the most common symptoms are fever ( 44% on admission and 89% during hospitalisation) and cough (68%). The median incubation period was 4 days. Another Chinese of 99 confirmed cases reported fever in 83% , cough in 82%, and shortness of breath in 31%. A few patients presented with muscle ache (11%), confusion (9%) sore throat (5%) and even chest pain (2%). Yet another retrospective analysis of 191 severely ill patients found that 94% patients had fever, almost 80% had cough, while 15% had muscle pain. An observational study of 36 children published 2 days ago reports that almost half of the children (mean age 8 years) were either asymptomatic or had mild symptoms. Common symptoms at admission were fever (36%) and dry cough (19%). I have presented these observational studies to underscore the commonest symptoms of patients with coronavirus are fever and cough. All studies have one thing in common where symptoms are concerned; a combination of fever and cough.
DOI: 10.1056/NEJMoa2002032
Crucially, no peer reviewed study to date has reported a patient losing the ability to smell or taste. But the world of otolaryngology is today abuzz with the terms “anosmia” and “ageusia,” An otolaryngologist is also known as an ear nose and throat doctor, or an ENT surgeon for short. And just about all of us have visited an ENT doctor at least once in out life time for symptoms ranging from a sore throat to to an ear ache, especially when we were children. Anosmia is the loss of smell, and hyposmia is reduced sense of smell. Smelling things that are not around is phantosmia. Ageusia is the complete absence of taste while dysgeusia is decreased ability to taste. It is important to get the definitions clear because of reports swirling around of a new symptom in coronavirus patients , who complain of loss of smell and even of taste. Anecdotal reports from many patients across the globe infected with coronavirus suffering from anosmia and ageusia have prompted the American Academy of Otolaryngology- Head and Neck Surgery and ENT UK to issue alerts about patients infected with the new coronavirus presenting with only the symptom of altered smell or taste. A detailed joint statement by the presidents of the Rhinological Society and ENT UK has underscored that there rapidly growing number of reports of proven patients infected with coronavirus losing the ability to smell, without any other symptom ascribed to the new virus. A significant number of Covid-19 proven patients have developed anosmia/hyposmia in China, South Korea and also Italy. Germany reports that 2 in 3 confirmed cases have anosmia. South Korea with wide spread testing has almost 30% confirmed positive cases having loss of smell as the major p[resenting symptom. In fact the UK statement documents the occurrence of 4 patients (all under 40 years) with only anosmia as the presenting symptom. But because these 4 patients had no other symptoms they did not merit testing or self isolation. Mention of these 4 patients in this statement becomes problematic because they are not coronavirus confirmed cases. The authors , very senior ENT professionals, are suggesting that anosmia be strongly considered , even if the only symptom, as a marker for Covid-19 infection. A person without fever, without any cough, or muscle pain, but developing sudden loss of smell should be considered a Covid-19 patient. She should be tested and also isolate at least for 7 days. The contacts of such a person should also quarantine themselves for a fortnight. Importantly the association of anosmia with Covid-19 underscores the importance of personal protection (PPE) of ENT surgeons, because they along with intensive care doctors and dentists are very much in the front line.
However it is imperative to appreciate that loss of smell is not an uncommon symptom in the community. A review of more than 5000 patients attending a taste and smell clinic for 4 decades , reported loss of smell in 87% and loss of taste in 62% of these patients. Remember these numbers are not of a community but 5000 people complaining of altered sense of smell or taste, evaluated over 40 years. Moreover these people were suffering from chronic smell and taste dysfunction, and were associated with post influenza type hyposmia and hypogeusia (27%), idiopathic or unknown causes (16%), allergic rhinitis (15%) and subsequent to head injury (14%). The researchers highlight the fact that the senses of smell and taste are vital for a fulfilling life albeit not in the same league as loss of sight or loss of hearing.

The UK ENT statement also clarifies right at the beginning that 40% of anosmia cases are due to viral infection. There are over 200 different viruses that can cause upper respiratory infection like the common cold or a running nose. Therefore it should not come as a surprise that the new coronavirus can affect smell or taste. The UK ENT experts however, based upon global anecdotal reports, warn that people developing sudden anosmia in the absence of other well known symptoms could be carriers of Covid-19, and should be isolated. The WHO so far has so far not added loss of smell or taste in their list of symptoms but are mulling over it. The British experts have been endorsed by the American Academy of Otolaryngology, who urge that anosmia or loss of taste, in the absence of allergies, sinusitis or rhinitis should warrant self isolation and testing. The American Academy recognising that loss of taste has been observed in patients ultimately testing positive for the coronavirus with no other symptom, has proposed “that these symptoms be added to the list of screening tools for possible Covid-19 infection.”
There are a lot of people with altered smell or taste because of reasons already mentioned, and not because of Covid-19. We already have a list of established symptoms in patients with Covid-19 that primarily include over and cough. Anosmia may become a marker in asymptomatic carriers but this will need confirmation in positive cases with Covid-19. To do that we have to start testing as many patients ,with sudden onset of anosmia or ageusia, for the new coronavirus; patients with only have anosmia or ageusia should be compared with a group of people who have absolutely no symptoms. Someone must have designed such a study Loss of smell or taste in a Covid -19 patient is not permanent; it usually resolves in 2 weeks. The mechanism for loss is still unclear; the virus affects the cells in the nostrils to the the olfactory nerve ( nerve of smell). However the insult is quickly rectified by regeneration of new cells.There is little or no taste without smelling. Eating delicious food is actually a combination of smell and taste.
Obviously Mr. Johnson has not noticed so far any alteration in his smell or taste . One should, in his position, retain the the ability to sniff out the best measures to tackle this pandemic, even as scientists across the planet strive to tackle the Covid-19 pandemic.
HOW BEST TO LOOSEN A LOCKDOWN ?

A significant amount of information was gathered by testing people for antibodies against the new coronavirus in China, Singapore and South Korea. The presence of antibodies against the virus indicates that the person has been infected and more over is now immune to repeat infection. Immunity top measles and mumps lasts a lifetime, whereas tetanus antibodies are present for a decade or so; thats the reason one needs another tetanus shot after 10 years. The first responders to the viral infection will be IgG (immunoglobulins G) that prepares the body for a counterattack against the invading virus. Next IgG (immunoglobulin G) come into play, they directly attack the infecting virus. The quantum of antibodies varies from person to person; some may achieve a large number of antibodies while others may produce a less robust response. Immunity to the coronaviruses producing the common cold or seasonal flu last a couple of years, and hence yearly vaccination shots against them; also the virus mutates, which means it changes its form to such an extent that the immune system fails to recognise it. And therefore the efficacy of the regular flu shot ranges from 40% to 60% only. Experiments done on monkeys suggest that immunity against the new coronavirus causing the Covid-19 pandemic does develop following infection. Antibodies against the 2002 SARS virus have lasted for a decade, and according to some immunity of some sort is present till 17 years.. Crucially antibodies formed by natural infection last longer than vaccines.
Testing for antibodies is called serological testing. The serological test identifies a person who has been infected with the Covid-19 virus but is NOT used to diagnose active infection. The antibodies can be detected as early as 3-4 days once symptoms develop and should stay for at least a few months if not longer. There is no data on duration of immunity against Covid-19 for the simple reason it is brand new evolving disease. Extensive serological testing have been done already in assign countries that has added to epidemiological data on the new Coronavirus. Germany has plans of testing hundreds of thousands people to ascertain the quantum of those infected. The state of New York has approved serological testing. Crucially detection of antibodies will provide a better picture of all those infected-symptomatic, middle symptomatic or without any perceived symptoms. A significant number of people will have to be serological tested, lets say around 10 lacks. This should not be too arduous because the test is substantially cheaper than the RT-PCR, and also gives results within minutes. PCR can take as long as 8-10 hours, while immune assay tests ( also used for diagnosis of virus presence not for antibodies) also give a result in a few minutes. The serological test uses blood while RT-PCR testing is done from swabs collected from the nose, mouth or lung secretions, and even from the rectum. But making the kits is not simple. Sections of the protein of the new coronavirus have to be produced in the laboratory to be used in an immune assay that detects whether antibodies are present. Expressing the protein in the right structure can be difficult. Which is the best protein to elicit antibody production? Most scientists agree the protein in the spikes of the virus are the best. The other protein is the nucleocapsid protein. It will be important to distinguish antibodies against common cold coronaviruses.
The serological test by identifying previously infected (symptomatic or asymptomatic) can be the best tool to decide on when and how to loosen a lockdown. The simple logic is that with serologic testing we can separate those who were infected earlier and now have the immunity to fight fresh infection, from those who were not infected and hence still vulnerable.All health personnel should be ideally tested to allow those with immunity to go back into the front lines. Similarly other vital components of the social fabric such as police, fire men, train drivers etc can resume work. The decision to reopen society, begin schools or colleges and get business back on track will depend upon knowledge of rate of infection and prevalence of immunity. Serological tests should not be used in symptomatic people because they would not have had the time to initiate an adequate response. Also clinicians understand that no test is 100% reliable, there could be both false positives and also false negatives. But this is all that we have in the given circumstances; there is absolutely no data from the US for the CDC to suggest an advisory. Most experts opine that immunity to the new coronavirus may be a couple of years.
However serological testing lakhs of people, albeit necessary will be a logistical and administrative challenge. The tests will have to be reliable and regulatory agencies will need to fast track clearance. But India can easily muster both muscle and cash for mass testing. The data acquired can become a model for other countries to help them implement their future strategies. Every country reeling under this pandemic is wondering when and how to unlock. Unlock we must, the loosening will have to be guarded and gradual. The decision will also depend upon areas reckoned as hot spots. Ten million people becoming jobless is less than a month in the US is most worrying. Serological testing will not be a panacea or some magic formula, it can determine the extent of the problem, it by itself will not stop viral transmission. The public has to follow the protocol of multiple hand washing, physical distancing, and sneezing ettiequte to combat the new corona virus.
Apart from giving some idea of the rate of infection in the community, and selecting people who can go back to work, the serological test can identify prospective donors. The concept of plasma donation by people who have a robust antibody response to very sick people has been done before. Plasma is what you are left with after separating the various cells in blood. Plasma contains antibodies and coagulant factors. Thus plasma has been administered in extremely ill patients with Hantaan and June virus (both produce hemorrhagic fevers), and also ebola. There are anecdotal reports from China that have successfully used plasma from previously infected people in severely sick patients of Covid 19. Recently a paper that included 5 severely sick patients treated with plasma was published in the Journal of the American Medical association. All 5 patients (2 women) were on ventilator support, 2 had fungal or bacterial pneumonia , and one patient needed extracorporeal membrane oxygenation (ECMO). All 5 patients had high viral load despite anti viral treatment.The researchers ensured that adequate IgG and IgM antibodies were present in the plasma, the antibodies were also checked for antiviral activity prior to administration. There was significant recovery in all patients, fever came down and ventilators could be disconnected. Body temperature normalised in 3 days in 4 patients while viral loads became negative ion 12 days. After 9 days of plasma transfusion 4 patients did not require a ventilator.Three patients have been discharged while 2 continue to be in hospital in stable condition. The authors conclude that plasma from previously infected people containing neutralising antibodies improved the clinical condition of 5 critically ill patients. They also correctly state further studies are needed to validate their findings. This is at best an exploratory pilot study. There was no control group that did not receive anybody loaded plasma. Hence it is not possible to say with certainty that the plasma administered was the magic bullet. It may be possible that the 5 patients recovered because of underlying anti viral and steroid treatment. The convalescent plasma was given upto 3 weeks into hospital admission, so we really do not know of the optimal timing with this intervention in patients infected with the new coronavirus. And most importantly the researchers acknowledge based on their data no conclusion can be drawn on reducing mortality by this treatment.
A study in 2004, on convalescent plasma in the treatment of 80 of 339 suspected SARS patients reported more patients were discharged on day 22 (58%) when convalescent plasma was administered before 14 days as compared to those given after 14 days (16%). Convalescent plasma was obtained from patients who had recovered from SARS.The plasma was given on an average 14 days following onset of symptoms because viral load peaks in the first week. The clinical deterioration that develops after a fortnight is due to inflammatory or hyperimmune response directed at lung tissue. There were no adverts effects because of plasma administration. Mortality in the 80 treated patients with convalescent serum was 12.5% while overall mortality in SARS patients in Hong Kong during that time was 17%. This study also was not randomised so definitive statements on plasma administration in severe patients could not be made; SARS was to soon disappear, so no large trial could be conducted.
But with Covid-19 it may be possible to conduct a randomised trial with convalescent plasma in patients infected with the new coronavirus. The pilot study published in JAMA, and previous research on other viral diseases suggest there may be clinical benefit with convalescent plasma. This needs to be confirmed. Serological testing should be done ,in the meantime, to understand better the infection rate of the new corona virus and to identify health personnel who could go back for frontline work in hospitals. The ICMR has pulled down its earlier advisory on use of serology in hotspots across India ( there are 20 of them). Kerala as per reports has begun using serological tests, while Haryana and Maharashtra are keen to begin. Around 8000 tests (PCR) were conducted today in India, the number of positive cases have risen to 2301, with 56 deaths. There are signals that domestic air and rail bookings may resume from 15th April in India, but they seem to be based more on empirical observation instead of hard scientific data.
The rest of the world there is scrambling to get serological kits by the millions, in order to pick out people who have developed immunity and can resume work. It is mandatory ,as explained earlier, that health workers be checked first to keep health systems up and running, and also that the rest of the population gets back to work. The ICMR has put up a skimpy advisory on antibody testing and also the names of the 6 non FDA/CE approved companies. Britain has ordered more than 17 million home kits knowing very well that the sensitivity in mild cases may be as low as only 50%, this rises to 90% in hospitalised patients. But the fact remains that it is imperative that we begin a serological program with greater zeal to define the prevalence of both disease ,and people with immunity to the SARS -CoV-2 virus. I cannot over emphasise how important it is to test for antibodies in the health workers ; those treating patients in intensive care units are well and truly in the front lines of one of the most unchartered diseases ever. Also, personal protection equipment of the highest standards, is mandatory for health workers confronting this virus on the front line.
LOCKDOWNS MAY NOT BE ENOUGH.
You can be certain the Prime Minister is quite aware that tackling the Covid-19 pandemic will take more that one day of self imposed quarantine by the public. He still has to be lauded for his efforts because in all probabilities he has sensitised the public of India to be prepared for future lockdowns of longer duration as was practiced in the Hubei province in China, and is currently being practiced in all the big countries of Europe. California is on lockdown for the next 3 weeks, it would be well to remember that the GDP of the state of California is greater than that of the UK or India. As of now California has 1,497 confirmed cases ( as reported by the Los Angeles Times) with 27 deaths. California is home to about 40 million people. Confirmed coronavirus cases have climbed to more than 25,000 in the US. Spain already on lockdown for a week will seek congress approval for another fortnight of lockdown. France too is under lockdown with orders of arrest and fine for non compliance. Italy with the highest number of casualties in the world was the first to impose nationwide lockdown in early March. But Lockdowns do not have universal support. The WHO’s chief emergency expert is on record stating that efforts must be made to find those who are sick, those who have the virus and isolate them, find their contacts and isolate them. He said this in a BBC interview with Andrew Marr today. The reasoning is simple; if strong health measures are not put in place the virus will just jump back after restrictions are eased. “Once we’ve surpassed the transmission, we have to go after the virus. We have to take the fight to the virus.” To tackle the virus it becomes imperative to diagnose its presence, and that can be done only by testing. Hence testing will have to be done in more and more people. To suggest that testing should be restricted to only the symptomatic or only the severely symptomatic is laughable. The fire cannot fought blindfolded. The excuse should not and cannot be that there are not enough testing kits. The Americans ate on the brink of producing kits that can confirm the corona virus in a mere 45 minutes. We too have to straight for the bones or the RNA in this instance of the virus. Maybe we could forsake a couple of Mirage jets and invest in production of testing kits. We could easily become the leaders and a model to the world. Resources are always to be handled pragmatically, but to suggest that one restricts testing as we have only 150,000 kits so far is more bizarre than scientific. Right now our hospitals are not overwhelmed by a deluge of coronavirus patients. We still have the luxury of time. There is however always the possibility that the virus will become uncomfortable as temperatures rise across India. Delhi is nearing 30C while London, Madrid, Milan and Rome are much colder. That the virus could be vulnerable to rise in temperature is pure speculation of course., one can only hope but prepare for the worse. The vaccine should take a year to be used in the public, keeping in mind that the common flu vaccine is only 40 to 60% effective for prevention.
There are so many Whatsapp messages rocketing around about Covid-19 nowadays, each as sensational as the headlines in Washington Post or the New York Times. I do not watch TV so have no information on Indian or ny electronic media. There is this chloroquine message that is piping hot. Apparently there is no chloroquine available with chemists in Delhi. Astonishingly there was not a strip of chloroquine available in my hospital’s pharmacy. There are authentic video clips in which president Donald Trump announces that the FDA had fast tracked its approval of chloroquine for Covid-19. Importantly the FDA denied this a short time later. The denial was necessary because so far there is not a single adequately powered randomised study on chloroquine in patients infected by the coronavirus. There are trials underway but not one has been completed or published in any peer reviewed journal. But a small observational study that is still not published compelled SpaceX founder Elon Musk to tweet that chloroquine was “maybe worth considering” as a treatment for Covid-19. Chloroquine has been used for the treatment of malaria since the 1940’s. The modern drug coms from the Cinchona plant, which was used by indigenous Peruvians for treatment of fever centuries ago. The trial that triggered president Trump’s statement on coronavirus in a press conference is based on only 20 confirmed coronavirus cases by RT-CPRl. The median age is 45 years, and no child below 12 years was included. There were 26 patients to begin with but one patient died, 3 patients required intensive care transfer, and 2 patients refused medication. Six patients were asymptomatic (17%) in this group of treated patients, the majority (61%) had upper respiratory disease (rhinitis or pharyngitis or isolated low grade fever with myalgia )while only 22% patients had pneumonia (confirmed by CT scan) or bronchitis. Sixteen patients in outside hospitals who served as controls were not provided chloroquine. A nasopharyngeal swab was collected every day to examine presence of the coronavirus. The treated patients were administered 200 mg hydroxychloroquine sulphate tablets thrice a day for 10 days. The primary endpoint was viral clearance at 6 days. Viral clearance was seen in 70% of treated patients on hydroxychloroquine but only in 13% of controls. Six patients in the hydroxychloroquine group were also given azithromycin for superadded infection; all 6 patients were virus free at 6 days. The authors of this paper concede that the number of patients are quite small in this study; that it was observational, follow up was short and 6 of 26 patients dropped out from the trial. An observational study of only 20 patients should at best be considered a pilot research; the findings of this study have to be confirmed by larger randomised trials; the FDA most certainly must be looking into this aspect. The WHO has so far not put its might behind this trial. There is no information about the 3 patients who had to shifted to intensive care. The patient who died on day 3 was PCR negative on day 2, the cause or manner of death is not explained in the French document.
Other researchers have begun trials with chloroquine. The University if Minnesota is one of them, it is studying the impact of chloroquine on people exposed to coronavirus. The results should be available in weeks. Till then chloroquine should not be bought over the counter, it should be administered in hospital settings by critical carte doctors. Quit the contrary has happened in Delhi, and probably the rest of the country. People have rushed to chemist shops to buy all the chloroquine available, without ascertain whether the drug works or not. It would be terrific if a randomised trial reported efficacy with chloroquine, its a generic drug costing a few Rupees. It can be manufactured by the millions by Indian drug companies. The University of Minnesota has also launched 2 trials with an angiotensin receptor blocker (Losartan) in patients with Covid-19.
DOI: 10.1056/NEJMoa2001282
Astonishingly little or no news has been reported by the mainstream media of a drug combination that actually significantly cut mortality in confirmed coronavirus patients. This was a randomised trials including 199 patients infected by Covid-19 in China. The fact that it reduced mortality from 25% to 17% has gone completely under the radar. The drugs are freely available in India. The NEJM published this trial on 18th March 2020. The researchers studied 199 patients with confirmed Covid-19 patients. The patients had to have severe infection; the oxygen sat on room air had to ne below 94% or they had to have a ratio of partial pressure of oxygen to fraction of inspired of oxygen less than 300 mm Hg. Patients were randomised to receive lopinavir-ritonavir (400 mg and 100 mg respectively) twice a day for 14 days, in addition to standard care or standard care alone. The primary endpoint was time to clinical improvement. The lopinavir-ritonavir cohort had 99 patients while the standard group had 100 patients. The researchers found that time to improvement did not differ between the 2 groups. Gastrointestinal side effects were common in the treated group but serious adverse effects were more common in the standard group. The authors concluded that hospitalised patients with severe Covid-19 did not benefit with the lopinavir-ritonavir combination. Future trials in severely infected patients may clarify efficacy with this combination. Lopinavir -ritonavir are p[rotease inhibitors used in HIV patients because they prevent virus multiplication. Now it is time to examine this randomised trial done in China carefully. This apart form being randomised is much larger; it includes 199 patients while the French trial had only 20 patients. The time to clinical improvement remained approximately 16 days in both groups, so no difference. The median age of patients was 58 years. The remarkable finding of this trial is the 28 days mortality, albeit a secondary outcome. There 28 day death rate was lower in the lopinavir-ritonavir group than in the standard care group for both intention to treat population (19% versus 25% ) and in the modified intention to treat population (16.7% versus 25%). A difference of absolute 8.3 % points lower mortality with lopanivir -ritonavir. Also patients in the untreated group and shorter ICU stay in the intensive group the standard care group ( 6 days versus 11 days). Also clinical improvement was at day 14 was higher in the lopanavir-ritonavir group (45% versus 30%). Respiratory failure, acute kidney injury, and secondary infection were more common in standard care patients. It must be borne in mind that the small French trial had almost 80% patients with mild or no symptoms, whereas the Chinese trial are far more serious with death rate of 25% in the standard care group. The trial was open label , meaning the researchers knew which patients were being treated with lopinavir-ritonavir, and hence susceptible to bias. Moreover 34% of patients also received corticosteroids and interferon (11%). An editorial tellingly asks why the drugs did not work, and provide 2 explanations. The population studied by the Chinese researchers were severely ill and hence challenging, as confirmed by the high death rate in the control group. Even advanced bacterial pneumonia is difficult to treat with the best antibiotics. Also the serum levels of lopinavir-ritonavir may have been lower than desired for optimal efficacy. However there was little difference in viral shedding with lopinavir-ritonavir despite reduction in mortality. But was the viral load detected adequate for further transmission is still unclear.
The mainstream keeps reiterating that more and more people are dying of Covid-19, sensational headlines appear every morning reporting of fresh deaths in different countries. As I write , the Economic Times reports that so far 7 people have died due to Covid-19, while there are 360 cases. The prevalence of coronavirus right now is 0.000269%, if the population of India is 1.34 billion.The mortality rate is 0.00000522%. Do the math yourself. 300,000 paeople have been infected in the world; 0.04% considering 7.7 billion people inhabit the planet.I personally am very sceptical of the mathematical models regarding the spread of the coronavirus disease; for instance 75% of Americans will be affected was the headline by yesterdays New York Times. India is still not under complete lockdown, despite many travel restrictions. A balance will have to be made between the transmit ability of coronavirus and the economic debility inflicted by long lockdowns. Also once a lockdown is imposed , the decision to relax or remove it altogether will depend entirely on a tight surveillance program involving identification, isolation, contact tracing isolation by testing and more testing. We must have some numbers to define the stage of the epidemic and we also need numbers for calling a lock down off. Too many lives are at stake to operate on whims and fancies. Spare a thought for the daily wager apart form the small businesses desperately trying to recover from the demonetisation strike. Also keep in mind the doctor in India unlike his western counterparts will soon have to distinguish Covid-19 from dengue from malaria from typhoid from chikungunya from common flu and from various common respiratory viruses. Not a small task by any means.
“BEWARE THE IDES OF MARCH”

Restaurants have been told to close down, small businesses are shuttered, cinemas have been shut, long haul air line sales are down by 50-70%, Apple has ordered all its retails stores (outside China) to remain shut for 2 weeks, world economy is down by more than 1.5%, in summary we are staring at recession. The economic battering is unprecedented, and quite real. The WHO has declared a pandemic that means a new disease is spreading around for which people are without immunity beyond expectations. Further a pandemic implies there are are cases in the community, not only from travellers from abroad. SARS was not termed a pandemic despite affecting 26 countries in 2003. Swine Flu (H1N1) on the other hand was branded an pandemic in 2009, bringing about considerable panic and overspending by governments on anti viral medicines. Covid -19 , a pandemic now, has triggered a media frenzy where main stream media is revelling in providing sensational headlines to further up the panic ante. The world seems to be coming to a swift end. Vlad Putin ,however, is least concerned as he is busy ensuring a life term for himself. Neither he or other Russians are particularly perturbed by the pandemonium reigning in the rest of the world. Trump tried his best to downplay the palpable trepidation and then suddenly declared a national emergency. Three Brazilians have tested positive for Covid -19, all 3 were present in Trump’s resort, in fact one of them sat on the same table as Trump. According to the White House Trump has tested negative and so has the Brazilian president. When more than 10,000 people die of a heart attack in a single day, more than 3000 people die of TB, and more than a 1000 people die of seasonal flu ( again in one day) why has the media whipped up such a frenzy? Covid-19 has been around since November 2019; but a mere 5000 people have died of it over the last 4 months. A single death by Covid-19 undoubtedly inflicts unbearable pain on the family, but then so does a heart attack. The Covid -19 storm is exceptional in its sweep. Why would Angela Merkel, a perfectly calm and composed leader, publicly announce that she estimates 70% of of the German population will be affected by the novel coronavirus. She had her health minster alongside her, and went on to add for good measure that there is no cure or vaccine for this plague. You have to terrify as many people as you can. What she conveniently missed out is that albeit millions will catch this virus, millions will also recover, in fact most will, especially those who are younger than 50 years. Japan has not recorded a single death under 50 years while South Korea is yet to report a death in any one below 30 years. The biggest data so far ( The Chinese Centre for Disease Control) has reported that no child less than 9 years died due to Covid-19. The American CDC is under a lot of flak for mishandling the outbreak , and is now scrambling to rectify matters. The American CDC had initially directed that only people coming from affected countries or those who had been in contact from such countries ought to be tested. Worse the kits provided for testing did not work.
Back to Trump. Why declare a “State of National Emergency” just a week after almost mocking the Covid-19 virus. Trump, good for him, never tired of informing the public that the WHO mortality figure of 3.4% was an overestimate for the simple reason the true denominator even today is unclear. We just do not know how many people are truly infected, many more people apart from confirmed cases must be moving around, these people may be mildly symptomatic or not at all symptomatic. A more reasonable fatality rate is 1% or less, but this will vary with age. Chinese data makes it clear that those above 80 risk 15% death, those in their 70’s are at 8% death risk, and those in their 60’s look at 3.6% fatality rate. The death rate falls below 2% in people in their 50’s. The South Koreans, who probably have tested the most people outside of China have documented a fatality rate of 0.6 to 0.7%. Italy reports a fatality rate above 5%, because one fourth of its population is above 70 years. Moreover Italian doctors are more than overwhelmed by admissions into their hospitals. The Italian College of Anesthesia, analgesia, Resuscitaion and Intensive Care (SAARTI) has published guidelines emphasising the need of prioritising patients on the basis of age and co-morbidities. The authors suggest that instead of providing intensive care to all patients, “the appropriate allocation of limited health resources” needs to be followed. ‘The allocation criteria needs to guarantee that those patients with the highest chance of therapeutic success will retain access to intensive care.” Also “It may become necessary to establish an age limit for access to intensive care.” Those too old to be considered to recover shall have to be scarified. Pretty cruel advice, but then almost al Italian banks are kaput, where do you get the pension funds from ? Do not permit children too visit their grand parents because them may infect them with Covid-19, isolate the old folks to despondency.
The new buzz word or mantra is “social distancing”, the severer the better. Do not venture out from your homes, do not meet any one, even dating could be a problem, your domestic helps may be infected, don’t drive to office, the metro logically is a potential threat to your well being, every place is shut down any way. No wonder airlines are in coma and the cruise ship industry is literally collapsing. Which begs the question that this virus was ensuring no oil is bought from the usual providers. Remember the most if not all American fracking companies have got bust, after having spent billions of dollars digging for oil from rocks. Exxon Mobil stocks are down by 40% despite 40 deaths so far in the US, most deaths were in. Nursing homes in Washington. To put in context as per CDC about 20000 Americans have died so far this year from common flu with 350,000 being hospitalised. Guess what. India still has only 107 cases, in a population that exceeds 1.38 billion people, and we also have the astronomical figure of 2 deaths due to the virus. Please bear in mind that of these 107 patients a substantial number have recovered. The Russians and the Arabs possibly in retaliation to the decline in oil requirements due to Covid-19 have crashed the price of oil to below 25$, and the Russians are prepared to lower it below 10$; annihilating American oil industry and also ensuring there is market for their oil. I mention the oil market and a mortally wounded world economy because there is more to this media frenzy about Covid-19. Every mainstream TV channel across the world is hell bent on scaring the hell out of the common woman and man with this virus. The virus undoubtedly is of concern, it can be transmitted to you, but it is not guaranteed to kill you. Catching Covid -19 is not a death warrant, a heart attack even in a person in his twenties could be.
I get the sense that even doctors have become caught up in the media storm. The coming weeks will demand that we keep are wits around us. Testing for suspected patients is mandatory as has been exemplified by the South Koreans. This should not be done in the Emergency Rooms, but ideally outside the hospital building under a makeshift shamiana. Swabs have to be taken by well protected personal. The more people get tested the lower will be the mortality rate, and lessen the fear will enveloping the general public. Only severely sick people should be promptly hospitalised and treated while suitably isolated. The mildly ill patients can be advised to stay home and employ common sense quarantine measures. In the event of worsening of symptoms the patient needs to get to the closest hospital. Hospitals will of course need to dedicate bets for Covid 19 patients, keeping in m ind that patients with heart attacks and heart failures will continue to come, so will patients with asthma and hip fractures who too will need urgent care. No hospital should be paralysed by only directing all its resources towards Covid -19 patients.
Tell you what, I have not seen a patient of Covid -19 so far, nor has any friend of mine got to know of one. They will come when they come; almost 20% of the severely ill patients will have cardiac problems that I have already discussed and will do so in the future. But I can write with great certitude that doctors in this country will not discard the old, come whatever. Even if our banks are bereft of pension funds. Crucially lets keep our fingers crossed that Mr. Trump does not get too excited with his “National Emergency”; he now believe it or not has powers well within US laws to modify or stop the internet, freeze bank accounts or even deploy troops to quell “rioting”. He is also now empowered to postpone the elections if he deems appropriate. Europe, which, is largely broke as of now already is mulling over martial law; but in fact thanks to Covid-19 this is already in place in quite a few countries. A tottering Deutsche Bank’s stock price plunged an other 15% last week. It is on the brink of collapse and more than a few obituaries have been finalised. No wonder Merkel was so articulate about Covid-19.
WASH YOUR HANDS, DON’T WASH AWAY A CONFERENCE.
The mindless slaughter of man and his business in North East Delhi is rapidly becoming old news, thanks to the Covid-19 virus that seems to have taken over the consciousness of the planet; reminding us on an hourly basis that these are not the best of times. Supply chains lie disrupted and global growth is anticipated to dip below 1.5%. Its never been so bad since thew 2008 crisis. Baselworld the biggest luxury watch event stands cancelled, it began in 1917 and has been held non stop every year; even through World War II. The Tokyo Olympics too is staring at postponement. The Japanese prime minister has been compelled to declare a state of emergency after a state of shock when Japanese bureaucracy badly mishandled the “floating petri dish” cruise ship crisis off its shores. No one wants the Olympic village to become a floating land petri dish. Despite the Feds lowering interest rates American stocks continue to stumble, and this certainly is not good news for the American president in an election year. Trump’s initial glee at Chinese manufacturing dip could leave him disheartened in the weeks to come. The simple reason being almost half of the world goods are made in China, and the Americans are in no position to hire Caucasians to sit in assembly lines making blue jeans or even iPhones. India imports around 60% of electronic components from China. There could be serious interruption impacting an already stuttering Indian economy. Elsewhere airlines stare at $113 billion losses because of aborted flights and this is considered unprecedented.
Conspiracy theories are swirling around. One that somehow the Chinese accidentally released the Covid-19 virus due to poor safe guard mechanisms. One of their biggest viral research centre is barely 300 metres away from the infamous wild animal market in Wuhan. After all the current hypothesis is that Covid-19 jumped from bats to an exotic wild animal and made a small step into mankind. China’s biosafety record is not exactly the best. Another conspiracy theory doing the rounds is that American soldiers competing in the Wuhan 2019 Military Games played some mischief, in the sea food market. Both conspiracy theories undermine international cooperation in combating the virus. Why is Covid-19 such a threat? Firstly because it is new and secondly we have very little data on its behaviour. We know it affects the elderly, people with chronic disease or impaired immunity. Mercifully children are less affected, why so we don’t know. It is still unclear as to how susceptible or how infective a school child is. Closure of schools therefore is based more on prudence than on science. Chinese men seem more susceptible than women, possibly because more of them smoke. Covid-19 has a taste for human lungs. Almost all scientists agree that Covid-19 has originated in wild life. They have the genome to prove their theory.
Almost 90,000 people have become infected and more than 3000 patients have died in China. That seems a big number but compare it to the seasonal flu. Flu has infected more than 3 crore people this season in the US alone. More than 300,000 have been hospitalised and around 18000 people have died. Fatality due to flu across the globe ranges from 300,000 to 600,000 in a single year; the fatality rate (percentage of people dying because of disease) is a mere 0.1%, but millions get infected by the seasonal flu virus. Seasonal flu unlike Covid-19 attacks children too. But the true fatality rate of Covid-19 is still elusive. There is absolutely no information available on the number of people infected but have no symptoms; also mildly symptomatic people will just not report themselves. Hence an authentic fatality number will take some time to be established. The current New England Journal of Medicine carries a paper with the largest Covid-19 patients studied. Of 1099 confirmed patients with Covid-19, 5% patients were admitted in ICU, 2.3% patients needed mechanical ventilation, while 1.4% died. Importantly only 1.9% had history of direct contact with wild life.Median age of patients was 47 years, and 58% were male. The most common symptoms were fever (89%) and cough (68%). Lymphocytes were reduced in 83% and ground glass opacity was the most common finding on CT chest (56%). Around 18% of non severe patients had no XRay or CT abnormality, and 3% of patients with severe disease. Crucially, if we keep in mind patients with minimal or no symptoms the mortality rate should be less than 1%, but when large numbers (in the thousands ) get infected the absolute number of deaths can be formidable. The case fatality rate with SARS is 9% and MERS is 36%. European leaders have been horrified by the lockdown of 11 towns in Northern Italy accompanied by orders of imprisonment if any one disobeyed orders. Another large Chinese study has reported that 80% of patients had mild disease defined as no significant infection of the lung, and about 15% had severe symptoms such as shortness of breath or low oxygen in the blood. Five percent of patients were critical requiring mechanical ventilation because of respiratory failure, septic shock or multi-organ failure. The WHO estimate of mortality so far is 3.4%, but this surely is an overestimate as it number derived from confirmed cases. The virus can be picked up from hard surface such as a seat in the metro, the virus probably lasts for 48 to 72 hours on a hard surface, but no is sure of the duration. The trick therefore is to wash hands frequently; wash your hands before you enter office or your home, and of course in between.
The Chinese Centre for Disease Control and Prevention (JAMA February 24,2020) reported that in more than 44000 confirmed cases mortality was 0% in children less than 9 years, but as high as 15% in those more than 80 years, and 8% in those patients in their seventies. Overall case fatality was 2.3%. Fatality was as high as 49% among critical cases.Most cases were mild (81% had no pneumonia or mild pneumonia) but 14% had severe disease ( breathlessness, respiratory rate >30/min, blood oxygen saturation 93%). 5% patients were critical (respiratory failure, septic shock, multiple organ dysfunction or failure).
Currently there is no specific drug against Covid-19.Trials are being conducted with remdesavir and Kaletra (an anti HIV medication) which is a combination of ritonavir and lopinavir. Ritonvir increases or boosts levels of lopanavir, helping lopinavir work better. Some researchers are of the opinion that remdesavir, which failed against Ebola, may prove effective against Covid-19. Preliminary results should be in by April. Remdesavir is a nucleotide analogue, which means it stops an invading virus from multiplying within the cell. Chinese doctors are experimenting with chloroquine hoping that because it is cheap it may be very useful in low income countries.
The reproduction (R) rate or the number of people a patient infects with COVID-19 seems to be about 2.2, in other words one COVID-19 patient is infecting 2 persons. The pandemic will go down when this number is pulled to 1 or less. The reproduction number for seasonal flu is 1.3.The race to develop an effective vaccine has begun but a commercially available vaccine will easily take more than a year to develop. The seasonal flue vaccine is effective in 40% to 60%n people. Till then the best preventive measure is cleaning ones hands with soap and water as much as possible. Sanitisers are sold out and masks are being sold at US $99 by some brands. The worth of a mask whilst walking on the road or driving ones car is of little value . Health personnel of course need to wear a mask especially if treating a patient with fever and cough. Unlike seasonal flu, Covid-19 does not cause a running nose, it has a fancy for the lungs.Mr Trump has gone on record that Covid-19 will retreat as the weather warms up. That may be true for the flu but we really do not know if the same will be the case with Covid-19.
Getting raw ingredients for common antibiotics and vitamins from China has become a problem, many factories over there are under lockdown. This has resulted in a struggle to manufacture these drugs by Indian companies. The government has urged or rather ordered the Indian drug industry to halt exporting 26 drugs and ingredients without its permission. India happens to export 20% of generic drugs to the planet. The government wants to ensure that enough drugs are available for the local population.
It is imperative that the scientific community ensures there is no panic in the general population. Clear information on Covid-19 must be disseminated in simple and lucid language. A brand new germ with the ability to kill people in the thousands is bound to install fear in the bravest. Something that cannot be seen or heard but can you are told lethally attack you is a frighting prospect. The message therefore should be repeated again and again that Covid-19 is a new virus, capable of infecting adults, a few seriously, but the death rate is bound to be less than 1%. The best that you can do is not to touch your face, and wash your hands. This virus has 2 strains, the L type that is considered more aggressive (found in 70% of patients) and the S type (30%) that is milder and the ancestral variety, but even this data is preliminary. The government of India and other governments need to invest more in health care, India’s budget contribution to health is a dismal 1.28% of the GDP (2018). It was a mere 1% in 2015.. Japan on the other hand spends 10.9% of its GDP in health care. The health care allocation in the 2020 budget is only 69,000 crore Rupees, which is 1% of the GDP. India is obviously ill prepared for a Covid-19 pandemic. Yet again the burden will be substantially shared by the private sector. Also claims that cow urine and dung is “helpful” against Covid-19 is patently false. Exercise, consuming a healthy diet, staying hydrated and having adequate sleep should keep ones immune system perked up. The best and only way to prevent spread of this virus is good personal hygiene. One cannot emphasise enough the importance of washing hands several times in a day, avoid touching mouth and face and keeping some distance from an obviously ill individual. Sneeze or cough into a tissue or the crook of your elbow, throw the tissue straight away into a bin.The Centers for Disease Control and Prevention (CDC) recommends self quarantine if you have mild symptoms, including mild fever and cough. But in case of high fever with shortness of breath consult a doctor. Do not believe that the virus is a hoax or not serious enough to isolate yourself. Do not fall for alternative treatment recipes. You have to alter your life style because Covid-19 will do what it has been designed to do regardless of your wealth, colour, caste or religion. It is not pseudo secular but actually very secular.It can however be contained by common sense and paying attention to health professionals rather than Whatsapp messages. YouTube videos on Covid-19 carry a link to the World Health Organisation; ‘Get the latest information from the World Health Organisation about coronavirus.” Instead of bashing heads in North East Delhi we have to beat Covid-19. Tuberculosis ,also spread by droplets, kills more than 15 lakh patients in a year, but TB is largely confined to middle and low income countries, hence the lack of appropriate reaction both from the Western and Indian media. TB affects 10 million or 1 crore people every year, so far 100,000 people have become infected with Covid-19. The latest New England Journal of Medicine has published a new drug regimen (of bedaquiline, pretomanid and linezolid) with 90% success rate in highly resistant lung TB, but there is not a whisper by the international media. Treatment success has never been better than 50% in severe drug resistant TB.

Instead of cracking skulls in North East Delhi, we have to beat Covid-19. This will not be possible by aborting conferences nor by closing down schools and universities, notwithstanding the fact that Covid-19 can kill. Crucially, when a vaccine or a proven anti viral drug does become available , it must be affordable for the general public and as Bill Gates has written not “sold to the highest bidder.”
HEMINGWAY WOULD NOT HAVE GIVEN AN OPINION ON THE RADIAL VERSUS FEMORAL APPROACH DURING PRIMARY PCI IN A HEART ATTACK PATIENT
“The best people possess a feeling for beauty, the courage to take risks, the discipline to tell the truth, the capacity for sacrifice. Ironically, their virtues make them vulnerable; they are often wounded, sometimes destroyed.”
Ernest Miller Hemingway
I watched the entire interview from beginning to end in great wonder. Here was this “senior journalist’ and great political expert explaining in excruciating detail how she converted form a fawning admirer to a deeply disappointed critic where the prime minister is concerned; all in a space of 6 years. In the beginning she considered him to be a comet against a dark sky, but now having turned geneticist she has grave concerns of the “DNA”. Astonishingly, she was blissfully unaware of the “DNA” 6 years ago. The distinguished interviewer with the nice bow tie kept milking her with questions that could only have one sided answers; there was no room for nuances. Having done the postmortem both almost lunged at each other to shake hands for business well done. After all a book is for sale. Now why would you take a book seriously by a “senior journalist” who in a span of only 6 years comes to a completely reversed impression of a man who never ever concealed his world view in the slightest manner? Anyone who has done the tiniest bit of serious reading knows where the world view comes from. The mindset was never kept under wraps. It was there for any and every dimwit to see. You may or may not agree with this ideology. Thats tour prerogative, at least for now. But for a working journalist to have professed public admiration and then equally publicly display anguish is a class act in itself. The good lady actually flinched when the lynchings took place. I certainly will not rush to buy this book. The only nice thing about the interview was there bow tie.
Contrast this with Hemingway. Hemingway still in his early twenties met a young Mussolini, and sent back his “ By Line”. Mussolini was a bluffer, wrote Hemingway. “If Mussolini would have me taken out and shot tomorrow morning I would still regard him as a bluff. The shooting would be a bluff.” He goes on “Mussolini isn’t a fool and he is a great organiser. But it is a very dangerous thing to organise the patriotism of a nation if you are not sincere.” Our prime minister beyond any shadow of doubt is sincere. The point I make is that it would be infinitely more worthwhile reading Hemingway than reading shallow books in search of sales. Hemingway repeatedly stated that what he wrote for his newspapers were quite distinct from his fiction prose. The former was to make a living while keeping in mind imposed dead lines; hence these columns may not withstand the test of time. But they have. Short sentences much like whiplashes minus grandiose adjectives was his style. Remarkably what he wrote as news continues today to be news. He wrote on facts but added what he felt. His editors did not object to the colour that he added to his columns. Crucially whether it was covering bull fighting, marlin fishing, the 2 World Wars, hunting, or even the luges of Switzerland , Hemingway had no axe to grind. He made sure he wrote true sentences. His grasp of economics and politics was immense and so was his ability to read human character. He blew his own head in the first week of July 1961, but is rated as one of the best writers of the twentieth century.
To more mundane matters. The radial approach versus the femoral approach during percutaneous coronary intervention; or ptca and stenting from the wrist versus there groin. I wrote a book on the radial technique and called it “Coronary angiography and Intervention by the Radial approach for Dummies.”( Kindle edition July 2013) The idea of the title that the radial approach was not that difficult; the book was published some years ago when less than 1% of operators were going the radial way. Rapid strides have been made since then; more than two thirds operators use the radial approach. The radial artery technique is associated with less bleeding complications, fewer puncture site problems and there has been a suggestion of lesser 30 day mortality. Above all, the patient can leave the cath lab walking if not on a wheelchair; with the groin puncture technique the patient has to stay lying down for almost 3 to 7 hours depending upon the procedure. A patient would prefer standing or at least sitting up soon after the procedure. There is however a slight problem for the operator; radiation exposure after all possible safe guards is almost twice with the radial technique compared with groin puncture. My initial enthusiasm has therefore waned , because I have been in the business of cardiac catheterisation since 1983; that is a considerable amount of radiation exposure.
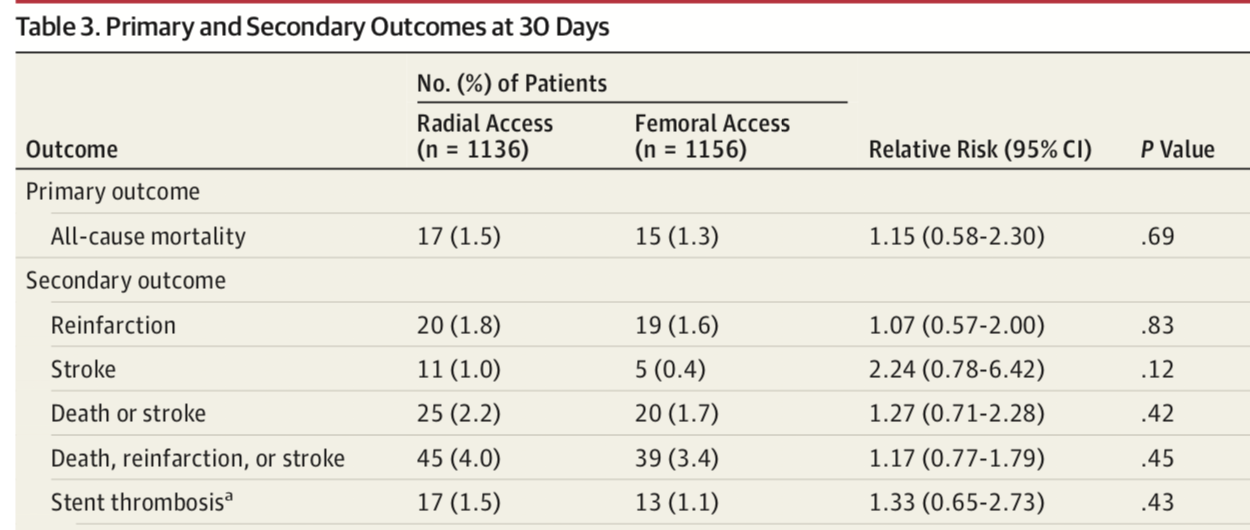
JAMA carries a large multi centric randomised paper comparing both these techniques in 2292 patients with ST segment myocardial infarction (STEMI). The researchers concluded that there was no significant difference for survival , nor any difference in rates of re infarction, stroke , stent thrombosis and bleeding.The trial was terminated prematurely. The reassuring implication of the SAFARI-STEMI trial is that adequately trained operators may obtain similar results regardless of puncture approach for primary percutaneous intervention in ST segment elevation heart attack patients. The results were consistent in all subgroups. Only 6% patients received 2b3a receptor blockers , while 69% in the femoral group got a closure device. The authors of 2 earlier trials suggesting fewer deaths with the radial approach gad underlined there need for confirmation.
The RIVAL trial including patients with acute coronary syndrome failed to show difference in mortality. But the sub group analysis of STEMI patients ( 1471in number) revealed significantly lower 30 day mortality with radial access (1.3% vs 3.2%), but the difference in deaths could not be explained by difference in bleeding (0.8% radial vs 0.9% femoral). The majority of deaths in fact occurred in patients who neither had bleeds or puncture site complication. It is presumed that bleeds translate to deaths due to accompanying hypotension or the necessity of stopping anti platelets and anti coagulants.
The RIFLE -STEACS trial studied 1001 patients with STEMI to report significantly 30 day lower mortality with the radial approach (5.2% vs 9.2%). Bleeding events were significantly higher in the femoral access group ( 12.2% vs 7.8%). But 2b3a receptor blockers were administered in more than two third patients. The MATRIX trial also could not show difference in mortality between radial access versus femoral access (2.4% vs 2.7%). The authors of SAFARI-STEMI rightly conclude that experienced operators in high volume PCI centres may get good and similar outcomes using either approach. But the 2017 European Society guidelines give the radial approach a class 1A recommendation; this obviously needs a rethink. One should be skilled in both approaches, and I for one make sure I take the a radial approach every now and then so that I do not lose the skill. Also there will always be a patient who would not be in position to lie down post procedure or who may wish to leave hospital at the earliest. But I like to cut down my radiation exposure by using the femoral approach. I doubt if Hemingway on being alive today would have provided an opinion, he would have stuck to his strengths and expertise.

PREVENTING OR TREATING A HEART ATTACK IN A COVID-19 PATIENT SHALL NOT BE EASY
The victory of the Aam Aadmi Party in the recently concluded Delhi election was more or less anticipated. This was clear from conversations with taxi drivers, auto-rikshaw drivers and petrol pump attendants. But let me confess I never imagined the scale of the triumph, this was more than an innings defeat in cricketing parlance ; The Delhi wallah whilst pressing the eVM’s , largely ignored the perforation of article 370, The Supreme Court verdict on Ayodhya and the call for identifying foreign nationals within the country. Interestingly while having lunch at ‘Haldiram’ yesterday I got into a gentle conversation with an absolute stranger, who claimed to be an eye surgeon in Birmingham or in other words an ‘NRI.’ The focussed good doctor not only continued to be in awe of Modiji but also revealed that a large group in Birmingham of which he is a member swore by Modiji. Obviously the Delhi woman on the street has other ideas. The eye surgeon to me was a classic case of reverse “ Blighty.” Blighty was the term used by British soldiers longing for home during the bitter battles of the trenches in World War 1. The young tired and famished English soldiers yearned for the peace and comfort of home. Nothing could compare with the horrors they were living days in and day out; admirably shown in the movie “1917.” Blighty implied a pastoral unspoilt home or England, of course imagined; but serious enough for the War Office to come up with a free magazine named “Blighty” for serving soldiers. And guess what Blighty was a mutation the Urdu word “vilayati” or foreign. Indians obviously termed British colonials “vilayati”, the Brits took up the word and dressed it up to “Blighty” meaning England. I have this impression that are NRI cousins do get more than homesick at times, or rather long for an imagined Motherland free of all inequality blemishes with a roaring economy. Sadly nothing can be further from the truth, but they can be pardoned as they are too far away to smell beneath the varnish.
Unlike the predictable Delhi election result, the COVID-19 virus play out continues to baffle both scientists and health workers. Yes the new name for the beta coronavirus is “COVID-19”, and the WHO has rightly rationalised this name as it does not hint at the geography or people involved; the name ensures there is no racial bias or stigma attached with it. International news is abuzz with COVID -19, each day brings out new figures and mortality rates. There was a surge in infectivity when the Chinese resorted to diagnosis using CT chest scans as opposed to CRP medical kits. The treason was simple , CT scans are quick in being done and getting reported, less than 10 minutes. The CRP kit that picks up the genetic signature of the virus can take as much as 24 to 48 hours for confirmation; worse reliability is also an issue. The CDC in the US swiftly realised that all CRP kits were not infallible. So far there have been only 4 deaths outside china, one each in Japan, Philippines, Hong Kong and France. France reported the death of an 80 years old Chinese tourist ; making it abundantly clear that the virus can be lethal in the oil and people with chronic illnesses like diabetes and heart disease. Their ability to fight back the virus is impaired due to a sluggish immune response, while children are better at combating this virus and consequently have mild symptoms.
Economists world wide have been quick to realise that the impact of COVID-19 that has resulted in lock downs in many cities of central China. Streets continue to be deserted, offices remain closed and people are justifiably nervous. The Chinese government is doing all that is possible to contain the epidemic and should be lauded as loudly as possible. I have not come across an article or edit in the Indian media that has expressed appreciation or admiration for the bravery of the Chinese people. Granted the Chinese army hammered us in 1962, but this is the time to express solidarity with the Chinese people and their government. There have no howls of protest or indignation by the common Chinese folks in deep conflict with COVID-19. Everything is off bounds, no weddings, no engagements, no parties, no playing football or just jogging around. What about funerals? You cannot mourn the dead, keeping in mind almost 2000 people have died. This may be a conservative number. There are bound to be more deaths till the virus dies a natural death by increasing temperature after some weeks. No vaccine is in sight, the earliest possible vaccine against COVID 19 will have to wait for at least a year if not longer. Moreover there is no guarantee that it will work in all. Most vaccines are effective only 65% or less of the time.
Offices are closed, as also factories. Tesla has closed down its factory, Apple reports that only 10 % of its workers attend office. China makes almost half all the world’s LCVD panels for TVs, laptops, and computer monitors. Apple has closed down all its retail stores and corporate offices in mainland China since 1st February. The biggest mobile phones conference in the world is the Mobile World Congress (MWC). It is to be held in Barcelona this year; Intel, NTT. Docomo, Amazon, LG , Ericsson and Sony have cancelled their participation. The conference begins on February 22. Samsung will have limited presence. The conference organisers have been compelled to ban all visitors from Hubei province, and will ensure all other visitors prove they have not been in China for at least 14 days. The global supply chain of a variety of products is bound to take a big hit. Particularly the drug industry, as China is the biggest exporter of raw pharmaceutical material. 80% of heparin used in the US comes from China. Heparin is an anticoagulant that is used in millions of patients undergoing coronary stenting and coronary by pass surgery. A substantial proportion of drugs manufactured in India depend upon Chinese supply chains., The American heparin is exclusively made from pigs and right now a swine fever too is raging in China and also Africa. No wonder the economic advisor in the White House has stated they anticipate a 0.3 % dip in this quarters American GDP because of the disrupted supply chains in China. Supply chains in supply chains need each other for raw materials. The Indian mobile phone that you carry should be having more than a few Chinese components. In fact the car you drive has 10,000 components assembled by the manufacturer but many of these parts were made in Chinese factories. An interruption in that supply chain is bound to be worrisome as would be a mitigation in medicine production.
And now finally to the heart. The COVID-19 virus infection is dangerous in people already carrying heart disease. The American college of Cardiology (ACC) has released a clinical bulletin regarding cardiac implications of COVID-19. The bulletin cites a recent report of 138 patients hospitalised with COVID-19 infection, and bases recommendations largely on this study published in JAMA a few days ago.Almost half of patients admitted for COVID-19 suffer from chronic medical illness, and these are the most vulnerable or susceptible to further complications. 40% of patients in the study already had a cardiovascular or cerebrovascular disease. In the 138 patients admitted nearly 205 developed acute respiratory distress syndrome, 17% developed arrhythmia, 9% came down with shock and 7% had acute heart injury. Around 4% had acute kidney injury. The first patient to die was a 61 year old chronic smoker who succumbed to ARDS and heart failure.
The guidance provided by the ACC is quite empirical and based on expert opinion. This is due to the fact that the COVID-19 epidemic is a brand new disease yet to reveal its full colours. New know as of now that it is highly infectious, spread by droplets that can remain infective on inert surface for 10 days. A person with underlying heart disease should be on high alert against COVID-19 as she should be against common flu, dengue and chickungunya. Every viral infection has the potential to spark an immune response that can actually backfire by destabilising plaques in coronary and cerebral arteries. Crucially harmful cytokines capable of damaging heart arteries are released. In the single centre study from Wuhan, China 26% patients had to be transferred to intensive care unit and 4.3% died. The common flu it should be noted kills around 1% afflicted. Both sexes were equally affected and median age ranged from 51 to 66 years.Almost all patients had fever while 70% complained of tiredness. One third had shortness of breath. Most patients received antiviral oseltamivir, and many were given antibiotics such as moxifloxacin, ceftriazone or azithromycin. Around 45% received glucocorticoids. Worryingly the authors note that many patients continued to be in hospital with unclear prognosis.
To me the ACC guidance is expectedly neither here nor there. There is no real data that increasing the dose of a statin or a beta blocker will in any way alter the natural course of the disease. Currently no antiviral has been found to work, and antibiotics are useless in a purely viral infection. The best preventive course is washing hands with soap and water as much as possible, and staying clear of suspected COVID-19 infection. Do I perform coronary angiography and primary stenting in a patient of COVID-19 presenting with an acute coronary syndrome such as ST segment elevation myocardial infarction? I have no data to back me up. For now each patient will require individualised care and loads of common sense. A rapidly changing disease profile will need further guidance but this appears improbable. Primary PCI in a patient with dengue can be the ultimate test, and so will it be in a COVID-19 patient having ground glass lungs on the CT chest scan. I certainly do not look forward to such a situation. Vaccination against the common flu would be sensible in order to reduce possible confusion between common flu and COVID-19 infection.
But we must empathise with the people of Hubei province and wish them well. I wonder if the government of India has offered any health care support to Beijing? If it has not there is still time to raise our hands; we should constantly endeavour to be on the right side of history.
DO NOT FEAR THE NOVEL CORONAVIRUS OF 2019
You must appreciate that more than 70 lakh people die of a heart attack in a year, almost 2 persons every second. No wonder so much rime and effort has gone into analysing the cause and management of this disease. The maximum number of research papers still deal with heart attacks. More people die because of a heart attack than those who died in the 2 World Wars, last century. Compared to heart attacks only 300 people have died so far because of the novel corona virus, or the 2019-nCoV. All deaths have taken place within China with the first out side death reported from Philippines this morning. This was a 44 years old man who had returned from China, was doing reasonably well the past few days but suddenly deteriorated in the last 24 hours and perished. He was diagnosed with “severe pneumonia” due to 2019-nCoV. There have been cases reported from other countries but no mortality. The situation however is fluid, we know little about the virus as of today. The clinical picture is evolving and the coming week will provide more information. Today it is clear that the virus has sprung from Wuhan, ion fact a meat market that sold just about everything that moved; including cats and wolves, pea cocks and rats, raccoons and snakes. The 2019-nCoV most probably resided in bats or snakes, and from there leaped into humans consuming wild animals or being in close proximity to them. But the virus has the capability of launching an attack on other humans who never ever visited the meat market that now has been closed down, in other words is is transmissible.

There is a report from Germany that a German male citizen (of 33 years) who had a business meeting with an symptomatic Chinese lady, came down with fever, sore throat, chills and muscle ache. His throat swab and a sputum sample confirmed that he was infected by the new virus. Quantitative reverse-transcriptase-polymerase-chain-reaction assay was employed for confirmation.Interestingly the Chinese woman developed symptoms on her way back to China. The German then infected another 3 colleagues . Fortunately all of them had mild symptoms, none came down with severe pneumonia. This means 2019-nCoV can spread from asymptomatic carriers. A person can harbour the virus, and yet may not develop fever or cough; but still infect another perfectly healthy person. The fact that there are symptomatic carriers of the disease means that we still do not know the true prevalence of the problem. Also the number of patents who will die is still unknown, mortality is still a moving target. But the clinical picture keeps getting clarified by the day.

THE LANCET
The study with the largest cohort of only 99 patients reports that the mean age of those affected was 55 years and 70% were males. Almost half of these patients had visited the notorious meat market of Wuhan. 2019-nCoV was confirmed by real time RT-PCR test that takes from 24 – 48 hours to get back. More than 80% of patients presented with fever and cough. One third had breathing problems. 75% had bilateral pneumonia while almost 15% had a ground glass appearance on chest CT scan. 17% developed acute respiratory distress syndrome (ARDS) and 11% of patients died of multi organ failure. There is one patient with pneumothorax.This is the highest recorded mortality so far; it matches that of SARS. The researchers emphasise that more men than women were infected, probably because women are more adept in fighting off infection by virtue of the X chromosome and their sex hormones. Also half of those infected by the new coronavirus had underlying diseases such as heart disease and diabetes. Older petiole with weaker immunity are more susceptible to 2019-nCoV.
In most patients lymphocytes ( a type of white blood cell) were reduced in number indicating that the new virus attacks them, especially T lymphocytes. The 2019-nCoV particles spread from lung mucosa into other cells and generate a variety of immune responses. Some patients rapidly develop ARDS and septic shock, followed by multi organ failure. Th researchers recommend administering intravenous immunoglobulin in severely ill patients; and steroids (methylpredinisolone 1-2 mg/kg per day). A low lymphocyte count not only is a prognostic marker but may also be used for early diagnosis in the clinic. Secondary infections included A.baumannii, K pneumonia, A flavus, C glabrata, and C albicans.
The only confirmed US citizen case is a 35 years male who visited his family in Wuhan, China. He complained of cough with fever for the previous 4 days.The patient was a non smoker and had no prior history off any disease. His chest auscultation revealed rhonci, but his chest X Ray was normal. His naso-pharyngeal and oropharyngeal swabs tested positive for 2019-nCoV by real time RT-PCR assay. The patient was hospitalised for persistent dry cough and 2 day history of nausea and vomiting. He however had no shortness of breath or chest pain. A stool test also confirmed 2019-nCoV infection by Rt-PCR but his blood sample was negative for the virus. He received supportive treatment. His white cells were low, and so was the platelet count. Liver enzymes were raised. Blood cultures were negative. A second X Ray showed pneumonia of the lower left lobe of the lung.The patient was treated with vancomycin (i gram intravenous 8 hourly) and cefepime( IV 8 hourly). The patient developed rhoncis while in hospital and so an antiviral was initiated ( IV remdesivir; a novel nucleotide analogue prodrug in development) on day 7 in hospital, with no adverse effects. The patient began recovering from day 8.
There are still many gaps in the understanding of this new virus, which the WHO has delved a global emergency. The virus was rapidly multiplying and transmitting probably all of November and December last year. The initial response by the Chinese government was tardy, but this may have been because of local bureaucratic inertia. But once officially reported on the last day of the last decade, the Chinese efforts have been stupendous. There has been swift transmission of data and information. A 1000 bedded new hospital has been constructed in a mere 10 days! This will function from tomorrow with 1400 health workers in attendance (from the military). Another equally large hospital is being made, to mange the imminent epidemic. More than 60 million people are still under lock down, their entry and exit shut down. A quarantine off this magnitude has not been witnessed before. It is a moot point whether this will stem the flow of virus transmission. The root cause needs to be tackled, this mandates a cultural shift, easier said than done. How do you convince hundreds of millions of people to stop eating wild animals. The meat markets selling wild animals have to be shut down forever if one seriously wants to prevent another novel virus outbreak. The WHO has done to declare global emergency, because if one third of patients need intensive care admission the best off health systems can be put under tremendous strain. The many low and medium income countries will just not be able to cope. Hence the disease needs to be contained with great vigour.
There is no need for panic. The army need not be called in. Common sense measures such as frequent washing of hands with soap and water will go a long way in prevention. Sneeze or cough in a tissue and throw it into a bin, avoid a manifestly sick person, consult your doctor if you have fever with cough, especially if you have come into contact with a person from China or a person who been in contact with a person from China. As they say constant vigilance is the price both of freedom and especially public health. So stay alert against any viruses of any kind, particularly viral tweets and Whatsapp messages that are invariably devoid of any science. Stick to the WHO for information or peer reviewed medical journals.
Explainer: Why the New Coronavirus Is So Dangerous

We now have about 3,000 confirmed cases worldwide, which is surely a conservative estimate.
The last day of the last decade provided the information that a brand new viral disease had emerged in Wuhan, China. Within a week, the new virus was recognised, which the World Health Organisation has named “2019-nCoV”.
Javadekar Doesn’t Think Bad Air Affects Mortality. Bad Air Does Much Worse.

Air pollution has been linked to depression, reduced cognitive function, dementia, brain cancer, chronic obstructive pulmonary disease and many, many other diseases.
The evidence is chilling. The time for blame-games is long past. There is also no need to point fingers because we’re likely past the point of no return. According to the latest WHO data, the world’s highest PM2.5 levels are to be found in India. We currently have 16 of the world’s 30 most polluted cities. These are remarkable figures that should surely be discussed fiercely on all TV channels every night.
2020 USHERS IN A NEW CORONAVIRUS AND THE CAA

2020 will be considered a seminal year for ushering in the new but deadly Coronavirus and the CAA. The silver lining probably is the new kid on the block number 4, Shreyas Iyer who has emerged as the number 4 batsman in limited over cricket by playing some breathtaking shots in consecutive innings against big teams such as Aussie ( in India) and Kiwis ( in New Zealand). Astonishingly the young man was not even thought of during the last World Cup inspite of a gaping black hole in the middle order. Importantly, Iyer ensured the Delhi IPL team reached the semis for the first ever time in the last IPL tournament, Delhi had all these years nestled in the bottom. There is captaincy potential in the lad; he without any doubt is a special talent.
The government has set the cat among the pigeons with the CAB and NRC. No Indian needs any elaboration on the acronyms, we have a raging bull in the China shop, only this time the shop is very much Indian. It is quite manifest the current rulers want to pulverise the constitution; they were absent when it was made; so therefore the onslaught now to make amends. Current thinking is not to care a hoot about minorities , women or the less privileged. If they had their way they would raze JNU, Jamia, and AMU to the ground and any other university that whispers any protest. Stephen’s too is up in arms. Few know the Quit India was almost launched from Stephen’s College. The then Vice Chancellor then mercifully looked the other way despite concerns of the Viceroy. The IIM’s and IIT’s have expressed their strong disapproval of the JNU fiasco, which of all things demonstrated the current dispensations penchant for cracking open heads of girl students. Gallantry at its best by the intrepid Delhi police.
The economy persists in lurching from disaster to another, it in fact is plummeting quicker than a tear-gas grenade hurled into a library. Hence, some learned chaps have cautioned us of diversionary tactics by the government. Divert and distract seems to be the current mantra of there government. But to fathom the working of the government it is critical that one reads up the biographies of Savarkar and Golwalkar, if not Doctorji Hedgewar. All three were very clear that Muslims at best can be second class citizens within the boundaries of Mother India, and that this privilege should be considered to be a favour. Christians too could settle for runners up if they were serious about settling in the local habitat. This is the core principle of Hindutva, that Hinduism is a more than a cut above the rest of the pack. Hence the brazenness in the current acceleration of transmitting the finer print in the party’s manifesto; comparable to the transmission of the new corona virus evolving from central China. A noted historian has rightly stated that our contemporary image abroad is mud or something to that affect. Not untrue, but there may be a tinge of exaggeration, for why would the West really care what transpires within our shores. They have their own problems, and serious ones at that. The Republic Day parade tomorrow will be watched by the Brazilian president who has gone on record that he wished all indigenous folks of Brazil should have been exterminated. A brilliant choice for chief guest; an amazing resonance of our current mindset.
The last day of the last decade provided the information that a brand new viral disease had emerged in Wuhan, China. Within a week a new virus was recognised, which the WHO has named “2019-nCoV”. I wish some one in the WHO had had the common sense to call this new virus “2020”, which sounds as deadly as the old “ 303” rifle the Indian soldiers had to employ in the 1962 Chinese conflict. 2019-nCoV sounds like an ISRO satellite. Any way the new virus has an RNA core and belongs to the corona virus family, corona means crown or the halo surrounding the sun. The arteries supplying oxygen to the heat are also called coronary arteries because the heart is considered the crown. This new RNA virus is called corona because under the electron microscope it is round in shape with spikes poking out from its periphery. Coronavirus are famous for producing that sniffling cold you get, but that is self limiting without any residual affects. The common cold by itself is benign. However, coronavirus have been incriminated in the severe acute respiratory syndrome or SARS, and also the Middle East respiratory syndrome or MERS. SARS carried a mortality rate of 10%, which is more than a heart attack treated in a city hospital. The mortality rate for MERS has been reported as high as 37%. The take home message is clear, the coronavirus is associated with considerable lethality. This is there reason the entire medical world is carefully looking at China. The Chinese have already reported 56 deaths, and more than 1500 confirmed cases. The mortality rate target is unclear right now, but is close to 5%, but this can vary for little is known about the toxicity of the virus or the response of a victim.
This week’s lancet carries the first clinical report that is quite disturbing. The cohort is just about 40 patients, of which one third landed up in the intensive care unit; and as many as 15% of these succumbed to the infection. Almost all patients present with fever, more than two thirds had cough and almost 50% suffered from weakness or muscle ache. More than half complained of shortness of breath. The paramount reason for breathless is the fact that this new virus attacks the lungs and not just the throat. Patients so far have not presented with a sore throat, the reason being that the 2019-cCoV launches an attack at the intraepithelial cells of lung tissue. 2019-nCoV not unlike other virus disease presents with low white cells and reduction in lymphocyte count, and raised liver transaminase levels.Where did this new virus suddenly come from? The internet is already awash with conspiracy theories that the virus already has a patent with a vaccine ready for administration. This is of course nonsense. The American Supreme Court has already declared that because virus are precent in nature there can be no patent for a virus sequence. Also there is absolutely no vaccine, neither is there a vaccine for SARS or MERS. The origin of the virus responsible for both SARS and MERS is the bat. In the case of SARS the concerned virus jumped from an infected bat to a civet and from that to humans. The MERS virus similarly vaulted from bats to camels and thence to humans.

January 24, 2020 https://doi.org/10.1016/ S0140-6736(20)30183-5
The New England Journal of Medicine has published a paper, which defines the genome sequence of the 2019-nCoV. The genome will go a long way to understand the origin and evolution of the virus. And therefore a step however small has been made to construct a vaccine. Interestingly there are reports that the 2019-nCoV probably also originates from bats. But the intermediary animal is as yet not known. Some scientists are pointing fingers at a Chinese snake or the cobra. Crucially ground zero is a sea food market in Wuhan that sells just about any meat, the Chinese have a very diverse and heterogenous menu. The lesson for now is to refrain from eating exotic meats.
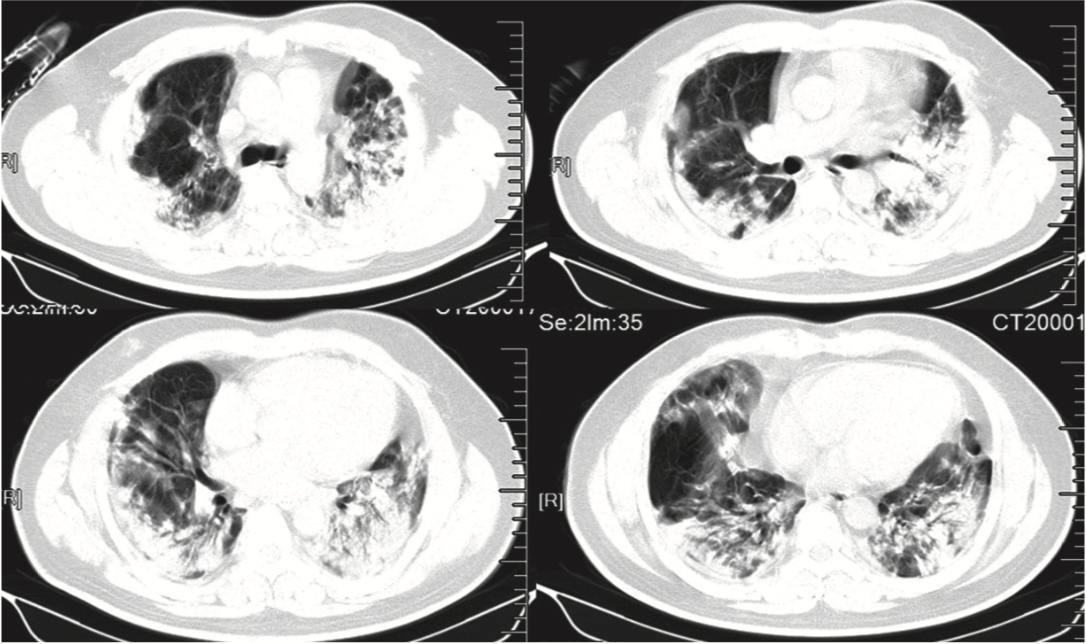
January 24, 2020 https://doi.org/10.1016/ S0140-6736(20)30183-5 ;LANCET
The 2019-NCov attacks the lungs with development of multiple pneumonia in both lungs. Soon the lungs adopt a ground glass appearance on a CT scan. This is when matters have gotten very grim for the patient can now die. There is no specific treatment, management being supportive. Treat fever with paracetamol, and when the lungs begin to fail intubate there patient and attach him to a mechanical ventilator hoping for the best. There is no proven antiviral treatment for the coronavirus. A combination of lopinavir and ritonavir did show some promise in patients with SARS, but this was in the lab and not in humans.A randomised study is being done in Saudi Arabia in patients with MERS ; a combination of lopinavir, ritonavir and recombinant interferon beta-1b versus placebo; the results are awaited. But no effective treatment has been developed for the new virus for obvious reasons, it is clinically less than a month old. The genome sequence has established birth of the virus as recently as October-November of 2019. The new virus genome sequence suggests its is 80% similar to the SARS virus. The 2019-nCoV virus has already been detected in Taiwan, South Korea, Japan,Vietnam and as close as Nepal. Cases have been reported from the USA and Europe. There is no reason to believe that 2019-nCoV is not already in India. We have scores of students studying medicine in China apart from people in the business community.

The WHO has swung into action by providing simple guidelines for prevention, wash your hands as often as possible with soap, stay clear of people with fever and cough, do not eat uncooked meats, if you have fever with cough and breathlessness consult a doctor as soon as possible. The new virus is capable of being transmitted from human to human, manifesting in global spread. Management is still unclear, but in the event of pneumonia admission to an ICU is warranted if not isolation. It was imperative that scientists, physicians, researchers and health workers crystallise a blueprint to diagnose, treat and contain 2019-NCoV. This is easier said than done; likewise the vigil regarding CAA and NRC will be a formidable task. The treatment for the latter understandably much more difficult. As for the 2019-nCoV infection, we now have 1600 confirmed cases, world wide, surely a conservative estimate. There have to be many more sub clinical patients, or those with less severe symptoms and therefore have not bothered to walk to a physician. Huwan is under lockdown, which implies no one is allowed to leave it unless there is an emergency. Railway stations and airports are closed. Two doctors treating patients with the new virus have died, one from a heart attack. Wuhan today is a ghost city. The Daily Mail (UK) carries a story that 90,000 people have been infected by 2019-nCoV in China.
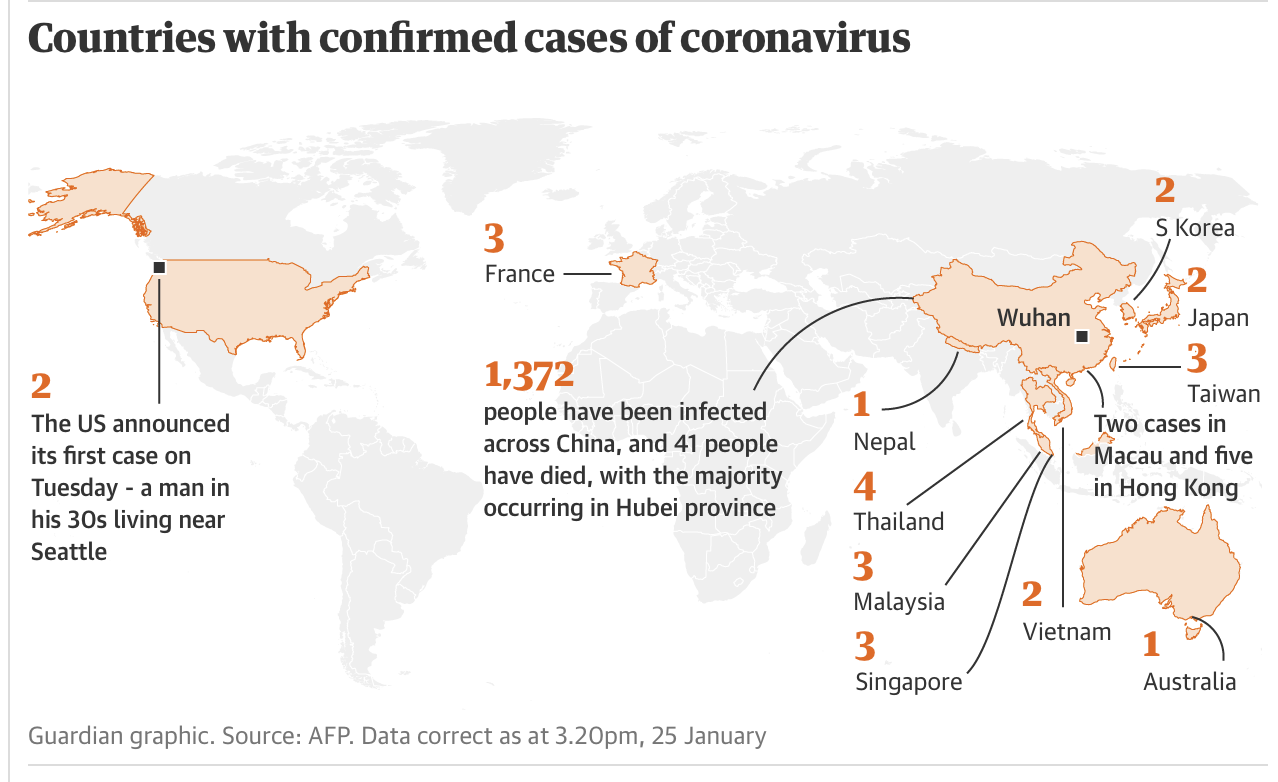
FALSE FLAGS AND THE GLOBAL SEPTIC BURDEN

There is something toxic with the Indian intelligence agencies. Its still too early to know how deep the rot is but it cannot be less than considerable. The question hovering around now is whether national security has gone septic now or whether it had been so for some time now. Even at first sight the arrest of Mr. Devinder Singh, DSP from Kashmir promises more than a sniff of a policeman gone corrupt. . Mr.Singh was remarkably nabbed ferrying not 2 but 3 terrorists in a car probably directed towards Delhi. Crucially the Republic Day is around the corner. Apparently the terrorists began their fantastic voyage form Mr.Singh’s home., a quaint coincidence. The Wire has reported that Afzal Guru had actually written a letter in broken English describing some strange events. Afzal Guru subsequent to being mercilessly tortured by Mr Singh, and coughing up Rupees 80,000 to him, was urged by Mr Singh to ferry Mr Mohammad (who did not speak Kashmiri) to Delhi. Afzal Guru was instructed by Mr.Singh to provide accommodation for Mr. Mohammad in Delhi, in fact Afzal Guru also helped Mr Mohammad purchase a car form Karl Bagh. The same Mr Mohammad was among the 5 terrorists shot dead in the Parliament Attack. Incidentally my Father was in Parliament that fateful day, and was quite unfazed when he got home. Afzal Guru wrote that both he and Mr Mohammad had mobile phones that received calls from our Mr Singh before the Parliament attack. The credibility of this letter is on thin ice because a man sentenced to hanging (until dead ) can clutch at straws. But Mr Singh has with great pride publicly acknowledged torturing Afzal Guru while the man was in his custody. Mr Singh was also posted in Pulwama, and till a few days before getting arrested was a part of the anti hijacking team at Srinagar airport. Why would a senior police man , an important component in the security apparatus of Kashmir , get conveniently caught escorting chaps from Hizbul Mujahideen? His chutzpah is breathtaking; it was as if he has been doing this on a regular basis; it is too audacious for a cop gone rogue. There is obviously much more than that meets the eye. It certainly a bit more complex than senior journalists attempting to tidy up the clutter around us. In the process they reveal their naiveté.
The Indian public knows little of “false flags.” Simply put the classic False Flag is to stage or actually attack one own asset, property or installation in order to agitate the public to the extent that people demand action. One of the first false flag operation was done by the Germans who attacked their own transmitter station, but alleged the Poles had done it; to subsequently launch an all out attack against Poland. The German people were indignant enough to egg their forces on with tremendous gusto; little realising a World War had been ignited, which ultimately would result in the death of millions and the ruin of Germany itself. The Japanese had staged a demolition job on its own railway to invade China, alleging the Chinese were behind the railway sabotage.
The Russians have been incriminated in a number of recent false flag attacks; the Russians are experts in false flag cyber attacks. Russian intelligence recently launched several hackings into 20 countries , mostly in the Middle East. Iran was the suspect but actually it was Russian intelligence , mercifully there was no attack against Iran then. The Russians probably never intended Suleimani’s assassination. A False Flag cyberattack is when a hacker stages an attack in such a way that the victim or people at large blame the state being framed.
Sony Pictures was hacked in 2014, with huge amounts of personal data being flung out in the open. The ‘Guardians of Peace” took initial responsibility but forensics finally figured out that the North Koreans were behind the hacking. Pro Russian hackers in Ukraine penetrated sensitive data of the (pro West) Ukraine government and also NATO to release information that deeply embarrassed the Americans and the EU. You have to admire the Russians, who took over an Iranian hacking team without the Iranians having a clue. “Tulra” (Russian)took over “Oilrig”(Iranian). The Russians were masquerading as Islamists. The Iranians were running a hacking ship minus their own flag but a fake flag; as and when possible they merrily cyber attacked vulnerable countries. Russian intelligence however penetrated the Iranian ship and used the Iran flag to assault whom they wished; the victims after rigorous investigation concluded the culprit was Iran ! What a False Flag by the Russian !Its not the Russians alone, the Americans and Israelis are equally adept and nimble with False Flags.
The New York Times published an Opinion piece on the bombing of 2 oil tankers in the Gulf of Oman. The Americans claimed the attacks were done by Iranians. The Iranians immediately issued a firm denial. According to the Americans Iranians had placed a bomb on the side of the oil tankers. They had video evidence of the dark deed. But careful scrutiny by independent security experts failed to confirm the American version. The opinion article highlights “The Gulf Of Tonkin incident.” The Americans had accused the North Vietnamese of attacking American destroyers in 1964, this enabled president Lyndon Johnson to persuade the Congress to permit escalation of American military intervention. Historians however have concluded that no American destroyer was attacked, it was a False Flag operation to ensure greater American military involvement in Vietnam. The 26/11 Mumbai attack was not a False Flag however much conspiracy theorists may advocate, because the government of the day did not stand to benefit in any way, moreover it did not, the dastardly attack in fact proved very embarrassing for the Congress party.
The Kashmir DSP’s arrest is a cause of concern; are we on the brink of further shock.Sepis is feared for exactly this, patients if not treated quickly enough go down the slippery slope of shock. Sepsis is the deranged and dysregulated life threatening response of the human body to infection, accompanied by acute organ dysfunction. The body begins to attack itself in defence against the infection. The risk of death is high, in fact in many cases more than an acute heart attack. Once the qSOFA score exceeds 2 or if 2 of 3 conditions are present the chances of dying become 10%; the conditions are 1)altered mental status, 2) systolic blood pressure less than 100 mm Hg or 3) respiration rate more than 22/min. The patient ism considered to be in shock if she needs inotropic support to keep mean blood pressure over 65 mm Hg or have serum lactate greater than 2 mmol/L. This week’s Lancet has published an excellent article reporting the global burden of sepsis. As expected incidence and mortality are greatest in low and middle income group countries, India has slipped into the low income group.
In 2017 almost 50 million or 5 crore people suffered from sepsis across Earth. Sepsis kills more people than cancer, and kills 5 times more people than treat cancer in America. Of the nearly 50 million sepsis patients more than 11 million or 1.1 crore patients died in 2017, that is every 3 seconds one patient dies (Lancet 2020; 395: 200–11).
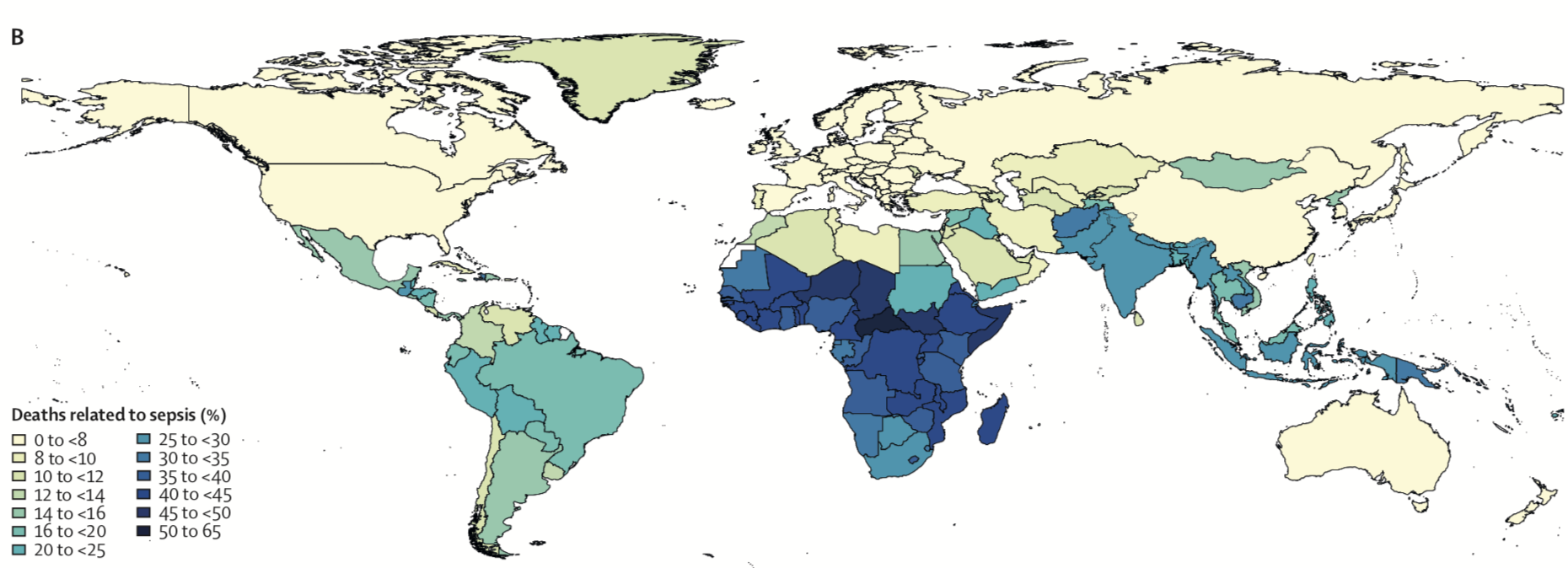
The incidence in 2017 is however less than in previous years, as there were more than 60 million cases in 1990. The recent figures rely own death certificates that may not be reliable, hence the figure of 50 million patients in one year could be a conservative estimate. The paper has been published by the Institute of Health Metrics and Evaluation at the University of Washington in Seattle. Half of the patients were children, the leading cause was diarrhoea for sepsis, while pneumonia caused most deaths. Recent guidelines underline the importance of sepsis being a harbinger of death that therefore mandates immediate response with broad spectrum antibiotics and intravenous fluids. Both gram positive (Staphylococcus aureus) and gram negative (Pseudomonas or E.coli) are responsible for most sepsis cases. The most important underlying cause was infection, followed by injury and non communicable disease.

The editorial applauds the first comprehensive world report on the epidemiology of sepsis; and urges that individual countries put up their own surveillance programs and protocols for treatment. Sepsis continues to be major cause of serious disease globally with there highest burden in low income nations.is not a disease but a syndrome that requires. Ironically the body mortally attacks its own organs while responding to an infection, a variant of a False Flag, bacteria frame the organs as the enemy, and the human body unleashes deadly chemical arsenal to destroy itself. Remember the bacteria has acquired its stealth after hundreds of million years of evolution; we are around a mere 200,ooo years old; puny compared to our co habitants of the planet. The bacteria hack is far superior to the Russians or the Americans; they delude us into believing that are own organs are the culprits, the result is total mayhem; the mother of all False Flags. No wonder 20% of all deaths in the world, due to illness, are because of sepsis. A victim , ladies and gentlemen, kicks the bucket, every 3 seconds.
SURGERY FOR ASYMPTOMATIC VERY SEVERE AORTIC STENOSIS AND THE KILLING OF CHILDREN

It happened more than a decade ago but even now seems odd that as thousands of Tamil Sri Lankans were being slaughtered during the last days of the Sri Lankan civil war no concern was expressed by any Hindu organisation within our borders. More 100000 civilians lost their lives courtesy the Seri Lankan forces is the conservative estimate provided by the UN and observers. It got queerer when Prabkakaran’s only 12 year old child was shot dead by Sri Lankan forces after providing him a snack a couple of hours before; not a whisper from our humble God fearing folks; after all is fair in love and war, including pumping 5 bullets in a 12 year old form point blank range. Maybe the Scriptures prescribe cold blooded killing of the children of your enemies. Conceivably the little boy and his mother had followed the tenets of the Roman Catholic faith. His mother too was cut down in cold blood. So was his sister.I wonder what spin our television and You tube savvy Gurus provided then or will deliver now, regarding the killing of the children. The Upanishads or the Gita do NOT endorse the murder of innocent children or women. Astonishingly and appallingly despite being the largest cohort of refugees within in our shores , Tamils who fled the worst possible genocidal onslaught in living memory are not included in the CAA. To add to their infinite misery the Rajapaksa are back in complete control of Sri Lanka.To many the CAA is fair game.

Let us recollect the high profile murder of of one of Sri Lanka’s most distinguished journalists, Lasantha Wickrematunge in January 2009. Mr. Wickrematunga wrote a remarkable editorial that was published after he was killed.”In the name of patriotism you have trampled on human rights, nurtured unbridled corruption and squandered public money like no other president before you,” Mr Wickrematunge’s editorial said to Percy Mahendra Rajapaksa. It was not uncommon for dissenting voices to be harassed , intimidated or even murdered in Sri Lanka as recently as 10 years ago. “When finally I am killed, it will be the government that kills me,” he wrote, in a more than 2000 word edit republished by the Guardian and New Yorker and attracted international scrutiny of the harassment faced by Sri Lankan journalists. Alas Lasantha who presciently wrote “I hope my murder will be not seen as defeat of freedom but an inspiration”, seems largely ignored by the Indian media. As far as I am concerned absolute and utmost respect to one of the bravest journalists the world has ever known. I would urge you, no beseech you to read Lasantha Wickremtunge’s edit ( freely available online). It is a must read in today’s times. His is a biopic worth making. His is a name worthy of being taught to every school going child on the planet.
“But there is a calling that is yet above high office, fame, lucre and security. It is the call of conscience. Our commitment is to see Sri Lanka as a transparent, secular, liberal democracy.” We need Lasantha right now and right here.
![]()
Now to an equally important subject. The commonest valvular disease in the Western world is aortic stenosis. All cardiac societies agree that severe aortic valve stenosis can only be treated by intervention that is surgical aortic valve replacement (SAVR) or trans catheter aortic valve replacement (TAVR). The intervention however should be done only if the stenosis has become severe and the person concerned is symptomatic. Symptoms consist of chest pain, shortness of breath or syncope ( giddy spell). The aortic valve is considered severe when its are is less than 1cm2 or the flow across the aortic valve exceeds 4m/sec or the mean gradient is more than 40 mm Hg. A small randomised trial from Korea published this week makes the case of intervening in patients who have not yet become symptomatic. This trial randomised 145 patients with very severe aortic stenosis ( defined as aortic valve area equal or less than 0.75cm2 with either an aortic jet velocity of attest 4.5 m/s or a mean gradient of 50 mm Hg), to early surgery or conservative care as currently recommended. The primary end point was a composite of surgical mortality (death due to surgery upto 30 days) or death from cardiovascular causes. The followup extended to 8 years. The primary endpoint was significantly greater in the conservative cohort, it was 1% at 4 years and 1% at 8 years n the early surgery group versus 6% at 4 years and 26% at 8 years in the conservative group. Sudden death had occurred in 4% at 4 years and 14% at 8 years in the conservative group. The researchers have concluded that the composite of operative mortality or cardiovascular deaths are significantly lower when patients with very severe aortic stenosis are treated by surgery even though they are asymptomatic ( N Engl J Med 2020;382:111-9).
The study will however not change current guidelines because a few caveats shall have to be kept in mind. Firstly only 145 patients have been studied, and all of them belong to the Korean peninsula. The average age of these patients is relatively young at only 63-65 years. Most patients undergoing TAVR are nearly 2 decades older; and being older carry the burden of other co morbidities or illness with them. None of the TAVR randomised trials have included patients with bicuspid valve, while the Korean paper has more than half the patients suffering from bicuspid aortic valves (54% in the conservative group and 67% in the early surgery group).

Randomised trials in patients with severe symptomatic aortic valve stenosis undergoing TAVR have reported equal if not better results in patients with low surgical risk, we therefore our moving into an area where TAVR can be considered a suitable alternative in almost all patients with symptomatic severe aortic stenosis. The age of the patient best suited for TAVR is still to be ascertained, because the life of the TAVR valve (tissue valve) is not as yet clear. TAVR is hence best suited in patients who have crossed their mid seventies because of the durability question; consequently TAVR in a patient in her sixties would be questionable.
The editorial on the Korean paper highlights the fact that 22% of patients in the conservative group never underwent surgery. So how does one best tease out asymptomatic patients with very severe aortic stenosis for surgery? That may be clarified by completion of ongoing large TAVR randomised trials such as “AVATAR”, “ESTIMATE”, and “EARLY TAVR”, which are trials comparing TAVR in asymptomatic severe aortic stenosis versus watchful waiting.
THE LEFT MAIN DISEASE TURF WAR BETWEEN STENTING AND CABG

![]()
Is Delhi burning? Not exactly but a couple of buses did get torched yesterday in south Delhi by angry protestors against the Citizenship Amendment Act. The Assamese too are more than irate at the new “Citizenship Amendment Bill “that was recently successfully thrust though the Indian parliament. Remarkably, there was little or no unrest while with National Register of Citizens exercise was going on in Assam. The affected folks were of course terrified.There was little to write home about after 19 lakh people were declared non residents or “illegal” occupants of the land. Even the realisation that of the these 19 lakh “illegal migrants” 15 lakhs were Hindus did not appear to cause great concern. The government however was obviously deeply concerned and swiftly moved into action. The “Citizenship Amendment Bill” got approved by both houses of parliament and shall soon be autographed by the president in Rashtrapati Bhawan. The citizens of Assam seem now to be acutely aware that the NRC exercise has served to purpose, they are back dealing with the same people they wanted out in the first place. Worse this time they shall not be dealing with “illegals” but those officially converted to “legals”, courtesy CAB. Small wonder the short lived sense of NRC relief has turned into a rage that has translated into violent protests, including the death of at least 5 people so far.
“The point is that it makes 200 million Muslims feel as if somehow their religion is not as valid or as Indian as the others. That’s not a good recipe for harmony.” That is Professor and Nobel Laureate Venky Ramakrishnan (2009 chemistry Nobel winner) on CAB in his interview to The Quint. He went on to say despite not being a local citizen he has “deep affection” for India and he wants ‘India to do well.”
It is impossible to be bored in modern India, every new day is an event. Probably diversion is needed from the mundane narrative of a rapidly declining economy, they say sales of both toothpaste and underwear are down; forget about selling a house. More than 10 lakh flats lie unsold in major cities of the country. There manifestly is no money going around and hence little appetite for consumption. Apparently unlike the Chinese economy that is based on manufacturing , Indian fiscal health depends on purchase. But what do you buy when you are broke ?

![]()
A much smaller seismic event has taken place in the world of cardiology with little notice by the Indian media. It concerns the left main (LM) coronary artery, which is the most important artery of the heart because it supplies good to more than two thirds of heart muscle. It divides into the left anterior descending and left circumflex coronary arteries. Blockage in the left main artery is of great concern because death is imminent if no treatment is provided. This is one blockage that mandates intervention either by coronary artery bypass graft (CABG) surgery or percutaneous coronary intervention (PCI) by stenting. Stents are tiny metallic tubes inserted into blocked arteries to make them patent. For many years CABG had been the only option for LM blockage or disease. Randomised trials done in the eighties of the last century had established superiority of CABG over medical treatment. The situation is much the same despite substantial improvement in medical therapy; left main disease can only be tackled by intervention; medicines do not work. The last decade however has witnessed the emergence of stenting as a viable alternative to CABG in the treatment of LM blockage or disease. Both American and European cardiology associations recommend PCI with stenting in LM disease of mild or moderate complexity based on the SYNTAX score, the recommendations are made based on clinical outcomes of high quality clinical trials. The first such trial to demonstrate equipoise between CABG surgery and PCI with stenting was the SYNTYAX trial, which randomised almost 800 patients of LM disease to CABG or stenting. The ten year long followup was recently published in the Lancet; the results suggested that mortality was the same whether a patient with left main disease underwent surgery or stenting. There was no significant difference in the death rate, even after 10 years.

![]()
The other big trial called “EXCEL”, however has become a huge controversy. The BBC beamed a documentary on accusations made by an author of the paper that vital data was concealed while publishing the paper in the prestigious New England Journal of Medicine journal. Professor David Taggart has been the “whistle blower” ; Taggart has withdrawn his name from the authorship of the paper because he believes that the incidence of heart attack has been withheld by the other investigators involved with the EXCEL paper. According to Taggart there were more heart attacks and more deaths in the stenting group as compared to patients undergoing CABG surgery, and that this data has been deliberately buried by the investigators of the EXCEL paper. EXCEL published its 5 years follow up recently, it recorded no significant difference in heart attack or death between CABG or stenting. Taggart’s allegations have been taken quite seriously by the European Association of Cardio-thoracic Surgeons (EACTS), which has gone to the extent of no longer supporting guidelines recommending stenting as an alternative to CABG.
The EXCEL trial was led by Professor Greg stone; it included almost 19005patients with left main disease; randomised them to CABG or stenting; and concluded that at the end of 5 years there was no difference in the composite of death, heart attack or stroke between CABg and stenting. Death of any cause occurred more frequently with stenting than CABG (13% versus 10%), but importantly definite cardiovascular deaths were similar (5% versus 4.5%). Heart attacks too were similar , around 10% in both groups. This is the data provided in the New England Journal of Medicine paper.

So how do we adjudicate the allegations made by Professor Taggart ( who by the way is a cardiac surgeon) and the BBC Newsnight investigation. Actually it is not too complicated. The problem lie not in the stars but in the definition of heart attack. You will be astonished to learn that even now there is no clarity as to what constitutes a heart attack. In simplest terms a heart attack implies that heart muscle is damaged to the extent that it is dead our necrotic; a small or large part of heart muscle gets damaged when an artery large or small gets completely blocked. One can therefore have a small or a large heart attack, which is measured by the amount chemicals or cardiac enzymes released by the necrotic heart muscle cells. The larger the damage the greater in quantum the release of these enzymes. There are largely 2 types of enzymes; creatine kinase MB (CKMB) and troponin (Tr). So far so good. The problem is that there is “Universal Definition” of heart attack and there is also a heart attack definition proposed by the Society for Cardiovascular Angiography and interventions (SCAI). The SCAI definition, to put it lucidly has a higher threshold or a higher bar; SCAI defines a heart attack subsequent to a PCI or CABG as an increase of CKMB ten times above the normal limit or a Tr increase by 70 above the upper limit. The “Universal” definition has a much lower threshold or bar to define a heart attack; the 2018 version defines a procedure related heart attack as a troponin level increase of 5 times more than the upper normal limit accompanied by ECG changes, 2 D echo demonstration of a new ischemic segment or the presence of (on coronary angiography) a blocked vessel, dissection of an artery or distal embolisation). So a heart attack is present with a lower bar when the “Universal” definition is employed; hence more patients will be classified as having a heart attack following a procedure. The SCAI definition on the contrary, with the higher bar, will identify fewer heart attacks. Professor Taggart and BBC Newsnight is deeply concerned that investigators of the EXCEL trial have used the SCAI definite and not the “Universal” definition, and therefore the allegation that had the “Universal” been used there would have been 80 times more attacks in the stenting group. These heart attacks were as explained involved a small area of the heart with little clinical significance. The Australian investigators reported that almost half of heart attacks using the “Universal”definition were due to occlusion of arteries < 1mm.
The response of Professor Greg Stone was swift; he put up a lengthy mail explaining the position of the Excel investigators. In a nutshell he emphasises the different thresholds of the 2 heart attack definitions. The riposte has already been explained by an elegant Australian study done a few years ago. The investigators of this trial used both SCAI and the Universal definitions in patients undergoing stenting. The patients were divided into a group with procedure related hear attack or a group without procedure related heart attack.They found that albeit more procedure related heart attacks were noted using the “Universal” definition than with the SCAI definition, at the end of 2 years the number of deaths or heart attacks were significantly greater with the SCAI definition ( 25% with positive SCAI versus 11% with negative SCAI). There was however no significant deaths/heart attack at the end of 2 years in patients identified as having stenting related heart attack when a rise in troponin was used (“Universal”). The Australian investigators reported that almost half of heart attacks using the “Universal”definition were due to occlusion of arteries < 1mm. Professor Greg stone in his explanation has underlined the fact that he and his co investigators considered the SCAI definition more suitable in the EXCEL trial. There was in the EXCEL trial no difference in heart attack at the end of 5 years with application of there SCAI definition. But the data on heart attack as per the “Universal” definition will be published also to further clear the air. He also made the point that the European association of cardiac surgeons should have sought an explanation from him before withdrawing from the left main revascularization guidelines.
The European Society off Cardiology however has not changed it’s recommendations regarding stenting in left main disease despite the BBC Newsnight investigation. Professor Taggart being a cardiac surgeon may be a bit sceptical about stenting and shall need to be satisfied by revealing the “Universal” heart attack numbers in ESCEL at the earliest. The BBC has pointed out that Professor Greg Stone has heaps of conflicts of interest. Stone is connected to nearly 20 stent/device companies as an adviser or other financial treated positions. The EXCEL rial was first presented at the TCT meeting , which one of the largest interventional cardiology conferences in the world. The TCT meeting is supervised by Professor Greg Stone , the lead author of EXCEL, and also millions of dollars are provided to TCT by nearly all major interventional cardiology product (stent) manufacturers of the world. EXCEL was supported by ABBOT , the maker of everolimus eluting stents used in EXCEL. Worse , one of the authors of the EXCEL paper has moved on to become the vice president of Medtronic, which is a giant stent manufacturing company. It will take some time for the air to clear; the issues involve life and death of thousands of left main disease patients.

It is important to mention a meta analysis of 24 prospective studies including almost 45,000 patients published in the current issue of EuroIntervention that concludes even 3 fold increase in troponin above the upper limit is associated with all cause mortality. The authors of this large meta analysis do not however discuss cardiovascular mortality; also studies that were included albeit prospective were not randomised. The editors of Eurointervention have issued a disclaimer that responsibility of the contents of this paper lies with the authors.
For now stenting should be considered for patients with the least complex left main blockage, and CABG surgery for more complex lesions; for the air to clear we may have to wait for another BBC Newsnight investigation. The SYNTAX trial is remarkable for concluding that even after 10 years there was no difference in mortality between stenting and CABG; and especially so because the stents used in SYNTAX were the paclitaxel eluting ones that are currently considered obsolete.
DIRTY AIR KILLS ; BUT DOES THE NATION WANTS TO KNOW ?
The evidence is surely chilling. The time to play the blame game is long past. Also, there is absolutely no need to point fingers because we probably have achieved the point of no return.The World Health Organisation seems rio have fixation for India. As per their latest data base , levels of PM 2.5 ( ultra fine particles smaller than 2.5 microns) are the highest in India. We currently have 16 of the world’s 30 most polluted cities. Remarkable figures that surely should be the discussed fiercely on all TV channels every night. Granted the dismantling of Article 370 and the majoritarian Supreme Court verdict on Ayodhya merit serious debate but the air around us is a killer. More people will die in this country each year than all the wars put together. Maybe even more than those slaughtered during Partition. Yet one does not perceive a proportionate outcry by the citizens of Delhi.Mercifully according to the WHO, the most polluted city on the planet is in Nigeria, a port named Onitsha. But Delhi cannot be far behind. Delhi recently bore the brunt of farm burning across adjoining states. The air quality was horrendous then, but is still potentially carcinogenic today. In fact I doubt there will be a single day in Delhi when we will be safe from bad air in the future. The population keeps rapidly climbing, construction work continues unabated and unchecked, and there is absolutely no solution for vehicular pollution. Ironically the slash in car and 2 wheeler sales could not have come at a better time, but the streets of Delhi are infested with traffic that churns out toxic air every minute of the day.
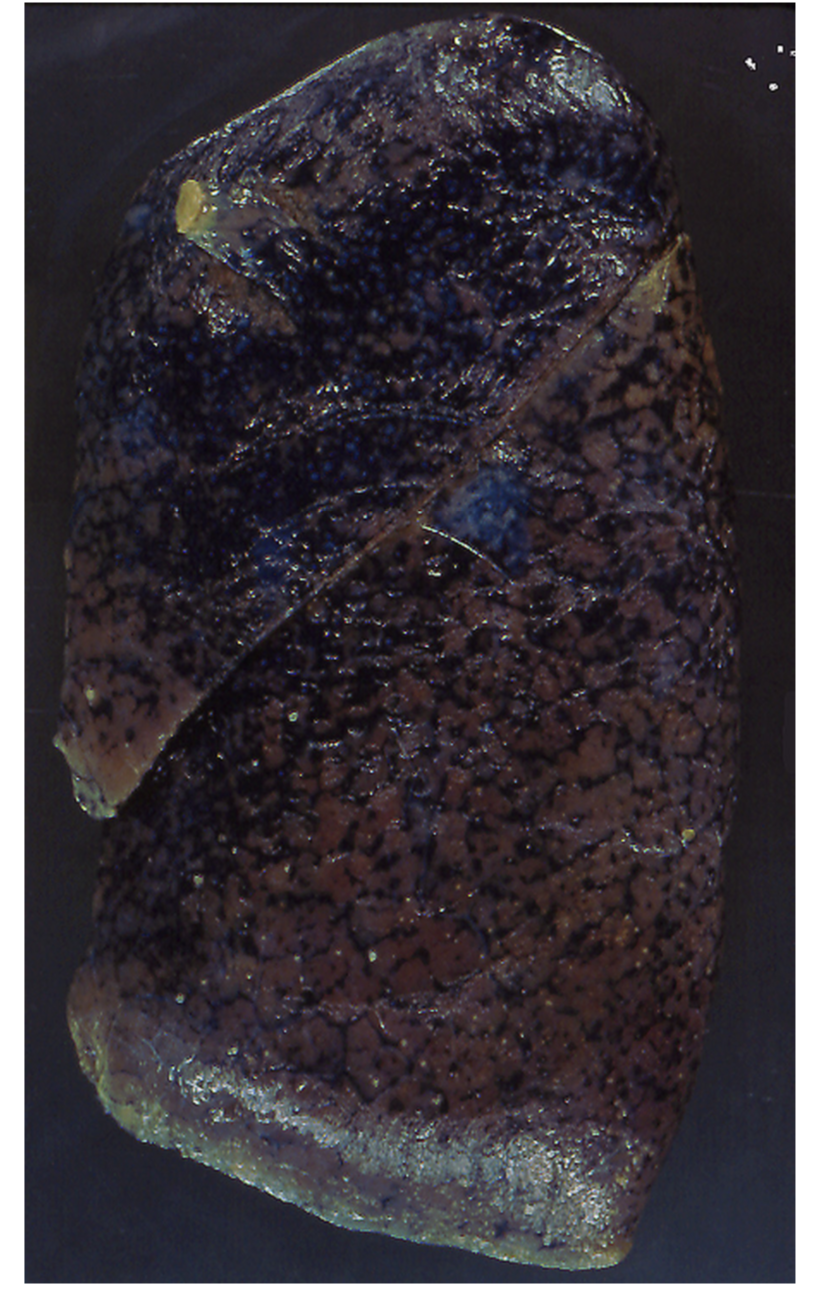
Somehow the consequences of bad air do not appear to sink in. We are indeed a stoic people, with the Mahabharata marvelling at the fact that we carry on living without the slightest acknowledgement of our imminent death. It has become a stale cliche to enumerate the horrible ways one can suffer by this toxic air around us. The list keeps increasing. We now know that just about every cancer in the body can be due to Delhi’s air because the 2.5 particles can affect every cell of the human body. It was already well known that bad air causes asthma, bronchitis and of course lung cancer. By penetration into blood these toxic particles affect the entire cardiovascular system; a chronic inflammatory condition is created. The person concerned becomes acutely vulnerable to high blood pressure, heart attack, heart failure and stroke. You are therefore looking at astronomical mortality figures. The biggest killer in the world continues to be cardiovascular disease, we are talking about more than 15 million deaths a year. A significant fraction of cardiovascular deaths are due to air pollution. The WHO is clear that air pollution kills around 7 million people each year. More than 80% people who live in cities monitoring air quality are exposed to toxic air around the world. The stats are staggering, while the response of people who matter in this country continues to be jaw dropping. As recently as August this year data showing independent associations between short term exposure of only 2 days to PM 2.5 and PM 10 ( particles 10 microns in diameter) and daily all cause , cardiovascular , and respiratory mortality has been published. The study included from m ore than 650 cities across the planet. A mere increase of 10 micrograms per cubic meter air in PM 2.5 and PM 10 was associated with a 36% increase in cardiovascular death and 47% increase in respiratory mortality. These mortality figures are from regions in the Northern hemisphere; the situation in India must be much more dire.

The connection between particulate air pollution and mortality was recorded as long as 70 years ago. There was clear evidence even then that number of deaths increased with higher levels of particulate matter (PM). The Dutch Environmental Longitudinal Study reported association of particulate matter pollution and mortality. Conversely the Chinese have very elegantly shown that bringing down particulate air pollution reduces stroke mortality. Air pollution ranked as the 11th most important risk factor of death and disability in the United States, while chronic obstructive pulmonary disease (COPD) is the third most common cause of death and disability. Crucially half of COPD patients have the disease because of poor lung growth rather than declining lung functions; every child in Delhi breathing toxic fumes is susceptible to developing chronic lung disease later on, part from having sub-optimally functioning lungs. There goes your future Olympic champion. Delhi had an Air Quality Index greater than 500 on 1st November 2019, that is 50 times more than the safe value of 50. The AQI was literally a stunner, because dear readers bad air adversely affects the human brain, by inducing depression, reducing intelligence and promoting dementia. Brain cancer too is on the list; it is a moot point whether dementia or brain cancer is worse.
We should be scrambling to tackle the mess we have created. This is not only a serious matter , it is downright deadly. Lakhs of lives are at stake besides increasing incidence of disabling and lethal disease. The problem is the public refuses to appreciate the looming danger. The time for the canary test is long past, right now Yama has comfortably settled himself in the largest sofa in the room, and he is larger than any known elephant. But he is not the one spewing out dirty air, for him it is collection time.
BIVENTRICULAR PACING. New England Journal of Medicine 2006
STENTING OR SURGERY FOR A BLOCKED ARTERY IS NOT NEEDED ALWAYS
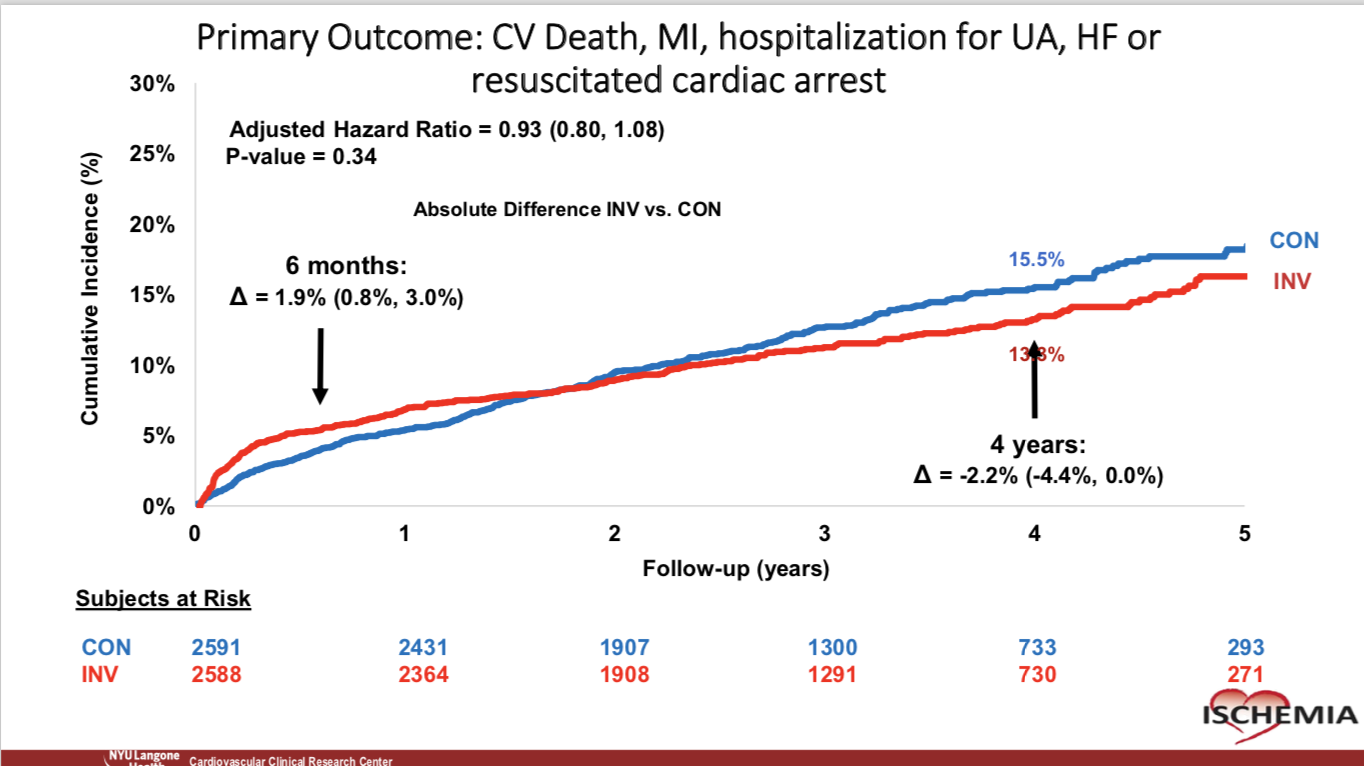
{kind=link}
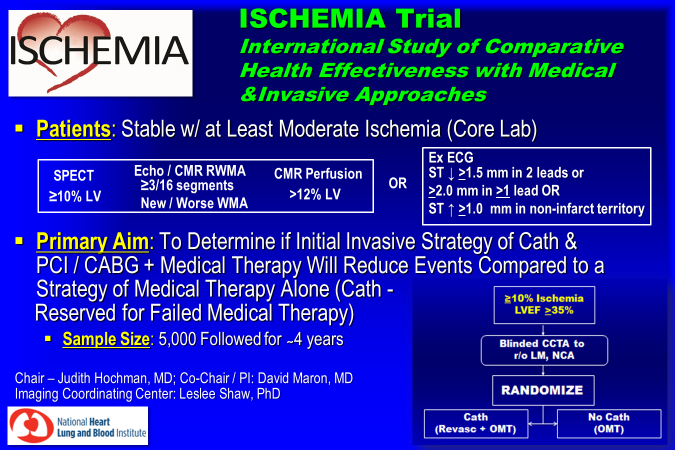{kind=link}
The much awaited ISCHEMIA trial was presented yesterday at the American Heart Association Meeting in Philadelphia, and the results were as anticipated by any common sense carrying doctor. Patients with stable angina , that is chest pain occurring only on walking, running or any other effort did not stand to benefit by coronary bypass (CABG) surgery or percutaneous coronary intervention (PCI) over and above optimal medical treatment (OMT). This was the important conclusion drawn by the 100 million dollars worth “International Study of Comprehensive Health Effectiveness With Medical and Invasive Approaches (ISCHEMIA) trial done over 10 years. This was by any standards a mammoth study and the inferences reached infinitely far important than the result of the current cricket test series between Bangladesh and India. In fact the ramifications of the ISCHEMIA study will be as sweeping and widespread as the Ayodhya verdict by the Indian Supreme Court, that has awarded the concerned spot of land for construction of a Temple and 5 acres nearby for a Mosque to be built. The judgment is clearly in tune with majority sentiment and despite mummers of deep concern is unlikely to be reviewed. The ISCHEMIA trial on the other hand just may be replicated but the results of the experiment will not change. There is little to achieve in incremental manner by coronary stenting in a patient of stable angina already on optimal medical therapy. Readers must be warned that the more than 5000 patients included in the ISCHEMIA trial had stable angina; they were NOT patients of acute coronary syndrome (ACS). They did not suffer from an acute heart attack or unstable angina, which is severe or moderate chest pain at rest occurring with increasing frequency. The importance of urgent coronary angiography followed by an appropriate intervention strategy (CABG or PCI) cannot be over-emphasised. Unstable Angina is a complete different ball game that needs rapid intervention, particularly in the case of a ST segment elevation myocardial infarction (STEMI).
The ISCHEMIA study included 5,179 patients with stable angina with preserved ejection fraction, in 320 sites in 37 countries. The patients needed to haver moderate to severe ischemia as assessed by a nuclear perfusion scan, almost 50% patients had severe inducible schema at baseline , 33% had moderate , and around 12% had mild ischemia. Patients were randomised to CABG or PCI over optimal medical treatment or to initial optimal medical therapy alone. Importantly, almost two thirds of patients underwent a blinded CT coronary scan to rule out left main disease or to confirm there was a block of at least 50% in other coronary artery branches. Patients with blocks less than 50% or blocks not accompanied with ischemia were also excluded. The patients excluded for left main blocks numbered 434, and 1,218 patients were excluded for having non critical disease. After a median of 3.3 years there was no significant difference in the composite endpoint of mortality, heart attack, resuscitated cardiac arrest, admission for unstable angina, or admission for heat failure, between the 2 groups. Patients included in the ISCHEMIA trial had inducible ischemia ranging from 5% to 10%.
Prior to the ISCHEMIA trial , the COURAGE study too had shown no superiority of an invasive strategy over optimal medical therapy in patients with stable angina. The COURAGE trial however was done more than a decade ago with most patients in the PCI group receiving bare metal stents, now considered inferior or obsolete. The ISCHEMIA trial had the advantage of some of the best stents in the business being used (cobalt chromium everolimus eluting) and the latest CABG techniques.
The take home messages are simple. Do not rush to coronary angiography if one is having stable angina with a normally contracting heart. Everet patient with moderate to severe ischemia need not sprint to the Cath lab.In the case of worsening frequency, duration and intensity of chest pain, especially if accompanied with impaired left ventricle ejection fraction, coronary angiography is the logical option. But what about the patient with a left main artery block who has few symptoms? Remember significant left main stenosis is helped only by early coronary intervention (CABG or PCI). But how does one rule out left main disease without undertaking a CT coronary angiogram ? The ISCHEMIA trial failed to show improved survival with coronary intervention as compared to optimal medical treatment but there was significant improvement in frequency of angina, and thereby quality of life. Along with the ISCHEMIA trial , results of the ISCEMIA-CKD trial too were presented; the ISCHEMIA-CKD trial also did not show any difference in clinical outcome s with PCI or CABG compared with medical treatment in patients with advanced chronic kidney disease and stable angina.
Normally a trial of the magnitude of ISCHEMIA gets simultaneously published in either the LANCET or the New England Journal of Medicine; but this however has not happened this time. Maybe the reason is that ISCHEMIA is a “negative” trial; but BIG PHARMA hardly stands to lose, it surely will enjoy greater sales, crucially justifiably so. The ISCHEMIA trial will eventually be published sooner than later, but November of 2019 will be be best remembered for the Supreme Court verdict in India and the ISCHEMIA trial presentation in Philadelphia. Also it is all very well to talk about optimal medical therapy, the reality is that only 41% patients in the ISCHEMIA trial were on high level optimisation therapy, despite careful follow up ! The lead investigator of the ISCHEMIA trial, Prof Judith Hochman, very rightly states that the “challenge in medicine is to get people to comply with their medicines and change lifestyles to reduce risk factors.”
To summarise this latest study did not find increased heart attack or mortality with medicines alone than in those who also received bypass surgery or stents. But if a patient continues to have chest pain despite optimal medicines, the person must consider a coronary angiogram. In India, a patient invariably lands up with the unstable form of the disease; stable angina can be, remarkably, ignored for months why the Indian people, much like the polluting air of Delhi is disowned and disregarded.