By Deepak Natarajan
Monday, July 23, 2007, www.tctmd.com
Operator(s):
Deepak Natarajan MD, DM
Affiliation:
Indraprastha Apollo Hospitals,New Delhi
Facility:
Departments of Cardiology
Indraprastha Apollo Hospitals, New Delhi, India
History:
A 58 year old male presented with non ST elevation myocardial infarction. He was a heavy smoker, but was not hypertensive or diabetic. The 12 lead EKG revealed ST-segment depression in the precordial leads and Troponin-T was positive. The previous day he had experienced near collapse accompanied by sternal chest pain and perspiration.
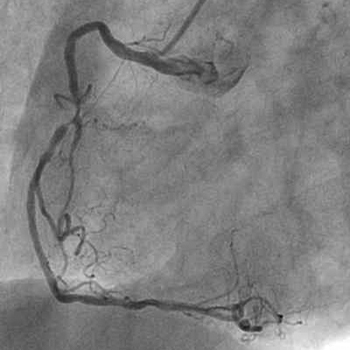
Angiography:
- 75%-80% proximal LAD stenosis.

- 70% proximal LCX stenosis.

- 90% stenosis of the mid RCA adjacent to the origin of a large right ventricle branch.
Procedure:
The left coronary artery was engaged with a 6Fr JL guiding catheter, and a 0.0014″ floppy guidewire negotiated across the LAD stenosis that was predilated with a 2.0x15mm balloon;  and an everolimus-eluting stent (Xience) 3.0x18mm was deployed at 18atm.
and an everolimus-eluting stent (Xience) 3.0x18mm was deployed at 18atm. 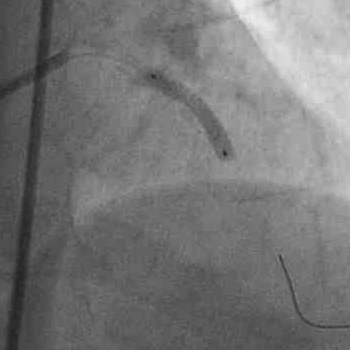 There was no residual stenosis and TIMI 3 flow was achieved.
There was no residual stenosis and TIMI 3 flow was achieved.  The same guidewire was then positioned in the LCX and the lesion stented with a bare metal ( Vision) stent 3.0x15mm at 18atm.
The same guidewire was then positioned in the LCX and the lesion stented with a bare metal ( Vision) stent 3.0x15mm at 18atm. 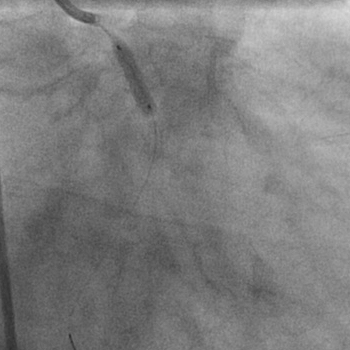 Angiography showed excellent flow into the LCX without any dissection.
Angiography showed excellent flow into the LCX without any dissection.  The RCA was next engaged with a 6Fr JR guiding catheter. Two floppy 0.0014″ guidewires were negotiated into the distal RCA and the right ventricle branch.
The RCA was next engaged with a 6Fr JR guiding catheter. Two floppy 0.0014″ guidewires were negotiated into the distal RCA and the right ventricle branch.  The RCA stenosis was predilated with a 2.0x15mm balloon; and a 2.5x18mm bare metal stent (BMS, Vision) was positioned across the lesion. Before inflating the stent, the guidewire in the right ventricle branch was removed;
The RCA stenosis was predilated with a 2.0x15mm balloon; and a 2.5x18mm bare metal stent (BMS, Vision) was positioned across the lesion. Before inflating the stent, the guidewire in the right ventricle branch was removed;  and the BMS deployed at 19atm.
and the BMS deployed at 19atm.  The final angiogram did not show any significant residual stenoses or dissection of either the main RCA or right ventricle branch.
The final angiogram did not show any significant residual stenoses or dissection of either the main RCA or right ventricle branch. 
Conclusion:
It was possible to achieve excellent flow in all 3 major vessels without any complications. The side branch of the RCA was not compromised. The patient was discharged the next day.
Comments:
The ARTS 11 and ERACI 111 studies comparing multivessel stenting involving DES with CABG have demonstrated comparable MACCE at follow up as for long as 3 years. The ARTS 11 trial used an average of 3.7 drug eluting stents with an average length of 73mm. The present case is an illustration of multivessel stenting utilizing one DES and 2 bare metal stents. the results were quite reasonable and there were no complications. Moreover, the tight bifurcation stenosis of the RCA could be managed with a single stent in the main vessel. The side branch was a little over 2mm; therefore, provisional stenting was never on the agenda, but in the event of significant residual stenosis or dissection of the side branch balloon angioplasty would have been possible. The SYNTAX and other ongoing randomized trials comparing multivessel stenting in 3 vessel disease with CABG should shed further light on multivessel stenting.
Conflict of Interest:
None