By Deepak Natarajan
Monday, August 21, 2006, www.tctmd.com
Operator(s):
Deepak Natarajan MD, DM
Affiliation:
Indraprastha Apollo Hospitals,New Delhi
Facility:
Departments of Cardiology
Indraprastha Apollo Hospitals, New Delhi, India
History:
A 59 year-old man was admitted to our service for unstable angina. He was a known hypertensive and had recently undergone an exercise ECG test which was strongly positive. He was not a diabetic and had stopped smoking a couple of years back. His LDL cholesterol was 150 mg%.
Angiography:
His coronary angiogram revealed a 95% bifurcation stenosis at the origin of the posterior descending artery (PDA) from a dominant circumflex coronary (LCX) artery. 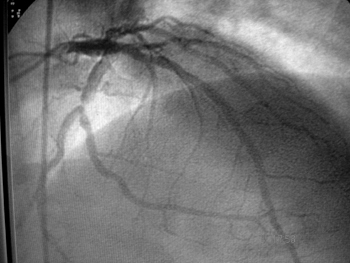 The left anterior descending artery (LAD) and the right coronary (RCA) arteries (non dominant) were normal.
The left anterior descending artery (LAD) and the right coronary (RCA) arteries (non dominant) were normal. 
Procedure:
The left coronary artery was engaged with a 7Fr Voda guiding catheter, and two 0.0014″ floppy guide wires were negotiated across the stenosis into the PDA and LCX arteries respectively. Following predilation with a 2x15mm balloon over both wires, a 3x18mm sirolimus eluting stent was positioned into the PDA while another 3x15mm sirolimus eluting stent was placed into the LCX artery. The PDA stent was placed slightly proximal to the LCX stent .  The LCX stent was first deployed at 14atm; and following a coronary angiographic injection, the wire was removed. Next the PDA stent was deployed at 14atm. The result was satisfactory with no complications.
The LCX stent was first deployed at 14atm; and following a coronary angiographic injection, the wire was removed. Next the PDA stent was deployed at 14atm. The result was satisfactory with no complications. 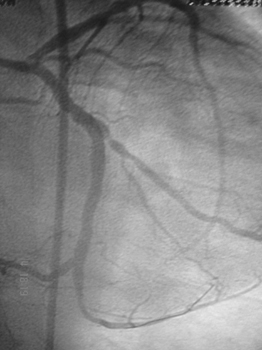 The floppy wire was renegotiated across the PDA stent struts and a 3x15mm balloon was inflated upto 16atm. Subsequent to this, kissing balloon inflations were performed.
The floppy wire was renegotiated across the PDA stent struts and a 3x15mm balloon was inflated upto 16atm. Subsequent to this, kissing balloon inflations were performed. 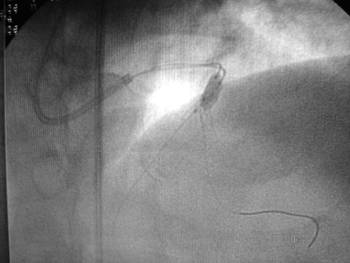 The balloons were inflated upto 12atm. Angiography revealed a significant dissection of the PDA distal to the stent.
The balloons were inflated upto 12atm. Angiography revealed a significant dissection of the PDA distal to the stent. 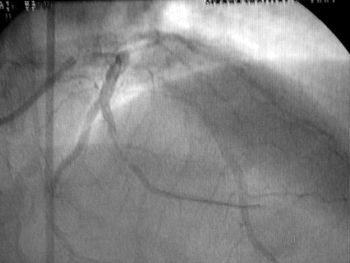 This was then predilated with a 2.5x15mm balloon and stented with a 2.75x15mm bare metal stent which was deployed at 16atm.
This was then predilated with a 2.5x15mm balloon and stented with a 2.75x15mm bare metal stent which was deployed at 16atm. 
Conclusion:
The final angiogram demonstrated TIMI 3 flow and no residual stenosis.  The patient was discharged the next day.
The patient was discharged the next day.
Comments:
Dissection of a coronary artery may develop following crush technique stenting. Although uncommon, it can be managed with deployment of an appropriate sized stent. In this case a bare metal stent was used for the sake of economy.
Conflict of Interest:
None