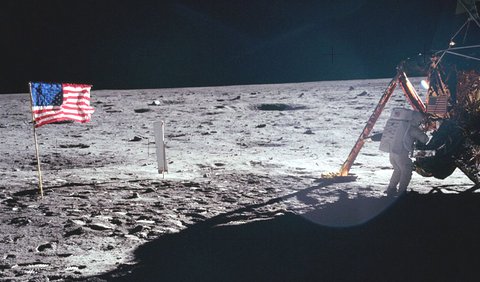
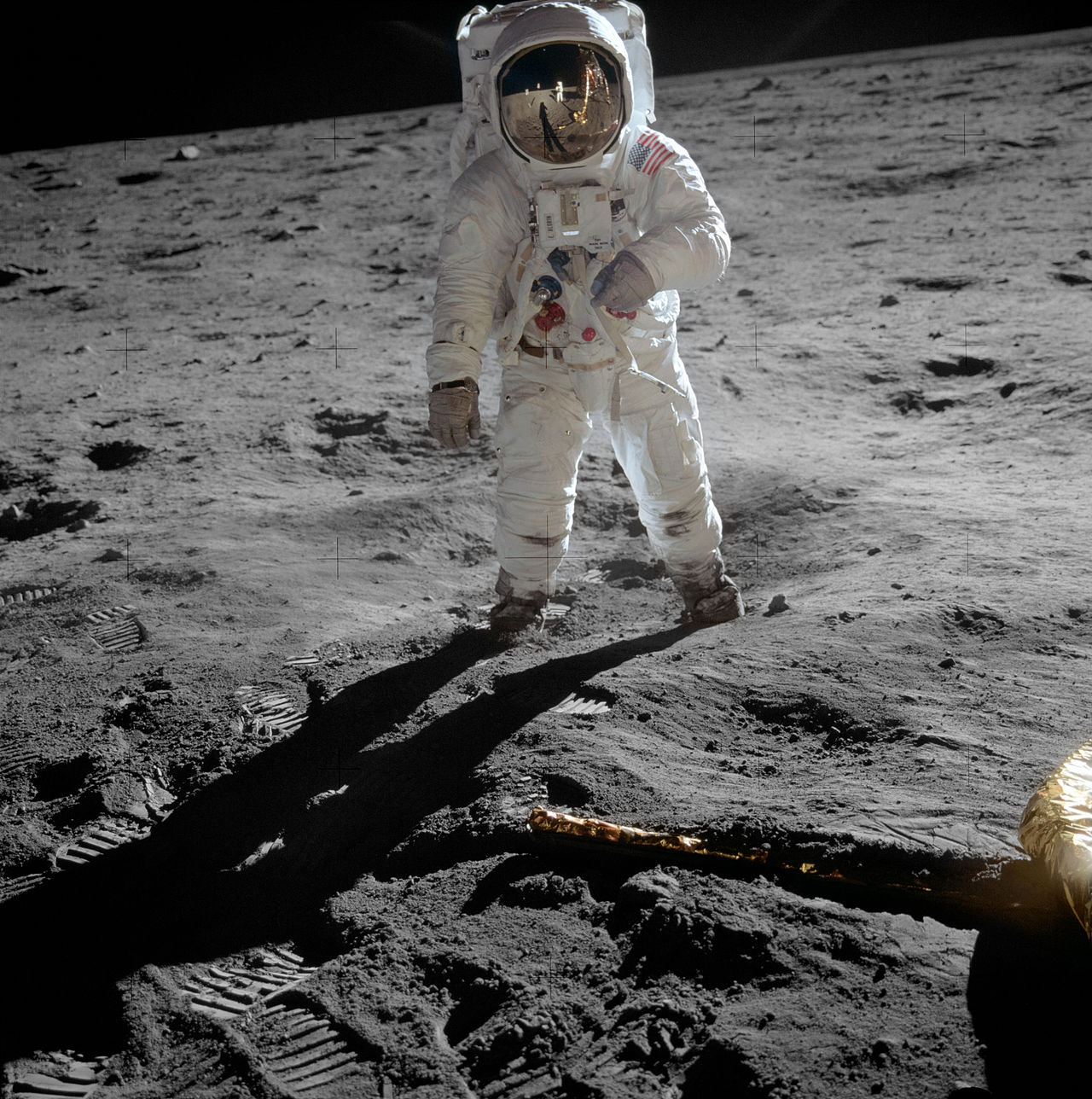
The first man to set foot on the moon was Neil Armstrong, way back on 20th July 1969. Neil Armstrong was an ace pilot and an engineer who supervised the Apollo 11 mission, which was the first space project to land on the moon. He became following this probably the most famous man on the planet. I still remember the grainy pictures beamed on our TV at home of him and Buzz Aldrin hopping on the moon’s surface. The famous line was uttered that “That’s one small step for man, one giant leap for mankind.” This was from more than 240,000 miles away. Possibly Armstrong dropped “a” before “man” or maybe he did not.
Just as famous was the line radioed back to mission control “The Eagle has landed,” when the lunar craft finally descended on the surface of the moon.
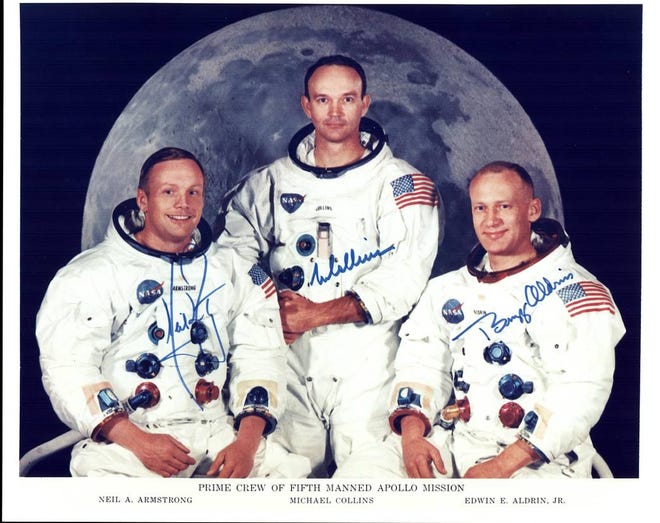
The Apollo 11 mission took off using a huge Saturn V rocket standing 363 feet. There is a documentary “Apollo 11” and also a terrific film “First Man” that has Ryan Gosling portraying Armstrong. Armstrong despite his immense fame did not care too much for grandiose pronouncements or striking statements powered by grand eloquence. Armstrong throughout his life remained a perfect gentleman with his feet firmly on the ground. This was an extraordinarily humble man right till the end. But what an end!
Few in India know that Armstrong died because of an easily avoidable error made by a nurse. Armstrong underwent a CABG surgery in early August of 20112. The surgery was unremarkable and Armstrong was recovering pretty well, he had even begun to walk following the operation. A nurse removed the temporary pacing wires attached to Armstrong’s heart in the ward itself. Sadly this tore apart heart muscle and there was instant severe bleeding into the pericardium (sac lining the heart) and hypotension. He was shifted to the catheterization laboratory where attempts were made to revive him, but had to be transferred to the operation room where all attempts at salvaging him failed. Armstrong lingered for another week before he died.
Temporary pacing wires are often attached to the surface either the right or left ventricle, and also the atrium. They are secured by a curve at the tip with or without a stitch. This is done during surgery. The wires are usually pulled on the 3rd to 5th postoperative days. Actually many surgeons prefer not to pul out the wires but just cut them on the surface of the skin. There is always the small risk that when the wires are tugged the heart wall can be ripped open, whether it is the ventricle or especially the atrium. Armstrong must have been on blood thinners ( aspirin).
Temporary epicardial pacing wires are placed to tackle postoperative arrhythmias that have the potential for hemodynamic instability. Pacing wires have been used to suppress atrial and ventricular tachyarrhythmias, as also as a safeguard in case heart rate drops after surgery. There may be rare complications, which can be deadly, as what happened with the first man to step on the moon. The most common complication is that the wires do not work when needed. Importantly removal of these wires can result in injury to venous grafts and tear of the chamber to which the wires are attached. The result is bleeding into the pericardium accompanied by a severe and sustained drop in blood pressure (also called cardiac tamponade).
Certain patients, however, may not require these temporary pacemaker wires, patients who undergo off-pump CABG, and those who already have a permanent pacemaker. There have been studies done trying to discriminate patients who could be at high risk for a temporary pacemaker. Diabetes and pre-operative arrhythmias are strong risk factors, and if the pacing was needed as the patient came off bypass. Most centers using bypass during CABG continue to place temporary pacemaker wires. Temporary epicardial pacing wires are also placed routinely during valve surgery, but high-risk patients can be teased out before surgery. Postoperative support if required is for 1 to 2 weeks.

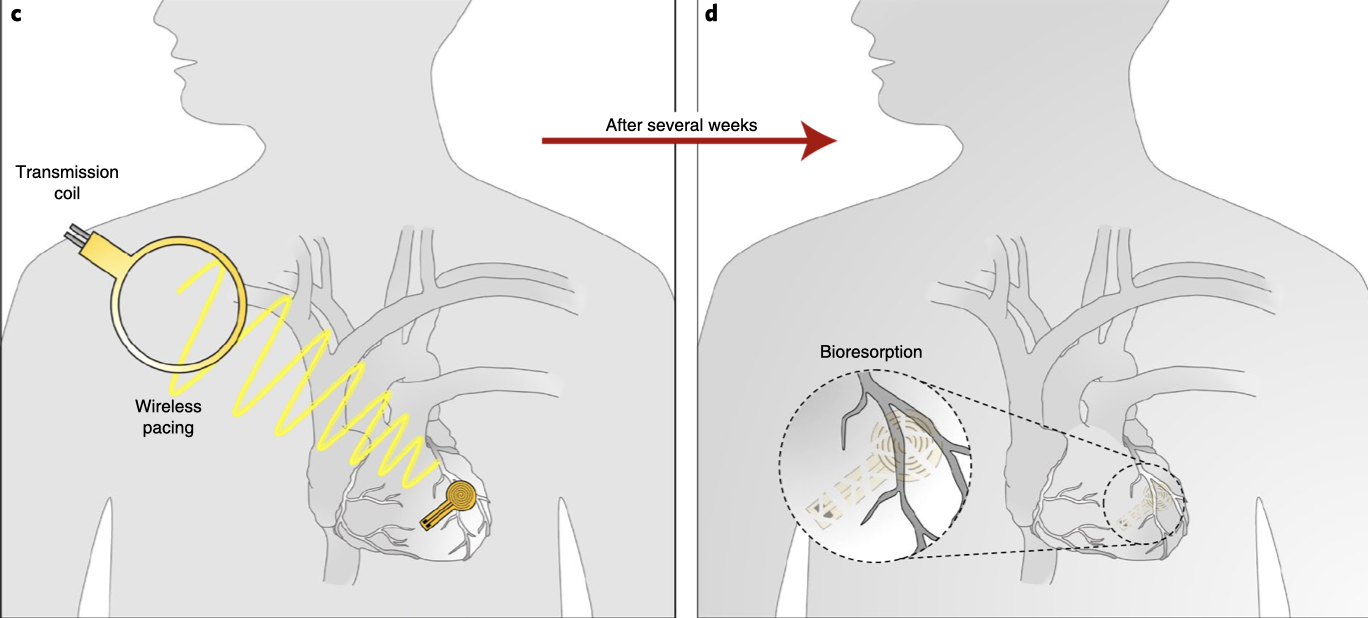
The good news is that now we are on the cusp of using a pacemaker that can dissolve within a month or two after the operation. A fully implantable, bioabsorbable pacemaker that can pace the human heart is being developed. Animal studies have been successful. There will be no possibility of infection or any complication during yanking of pacing wires. This device is very small and made of water-soluble biocompatible materials. It has no wires or battery. It will do its work of protecting the patient from possible arrhythmias and melt away. The device is 16 mm in width, 15 mm in length, and weighs just 0.3 g. The device is capable of receiving commands and power from an external source on top or a few inches from the heart. It has successfully captured and paced rabbit and mouse hearts. The pacemaker largely dissolves by 3 weeks and almost completely by 12 weeks.
The dissolving pacemaker is stitched on the surface of the heart and therefore there is no risk of a residual fragment traveling in the bloodstream. Human trials are eagerly awaited. The future looks promising but one must bear in mind the usual caveats of suboptimal effectiveness and unanticipated adverse effects. Till then we will have to continue with the temporary epicardial pacing wires attached to an external generator.
The richest man in the world , Jeff Bezos, went up 65 miles above Texas ,yesterday. It was a gigantic unadulterated ego trip lasting 11 minutes, even as millions on the ground stared into a dark abyss infested with the Covid 19 virus.