By Deepak Natarajan
Monday, July 12, 2010
Operator(s):
Deepak Natarajan MD, Hakim Udin MD,Nirmalya Mukherjee MD and CK Krishna MD
Affiliation:
Moolchand MedCity, New Delhi, India
Facility:
Department of Interventional Cardiology
Moolchand MedCity
New Delhi, India
History:
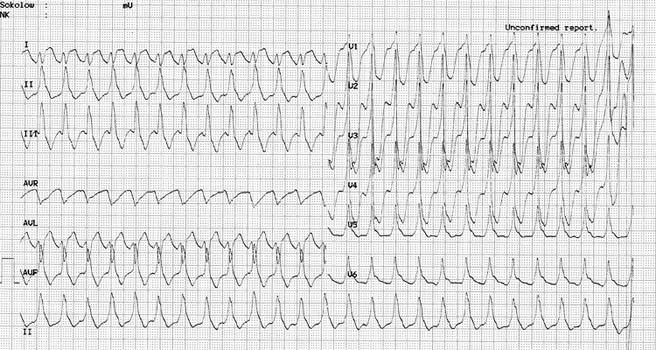
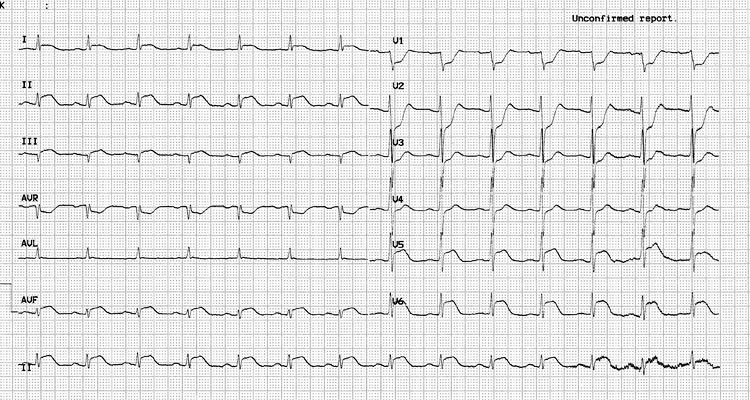
A 76 year old non-diabetic, non-hypertensive man was admitted in the ER for central chest pain for the previous hour. His 12 lead ECG revealed a sustained monomorphormic ventricular tachycardia at a rate of 150 to 160 per minute of right bundle branch morphology (Figure 1, Figure 2). He maintained a systemic blood pressure of 90 mmHg. On reversion to sinus rhythm by 2 bolus injections of 150 mg amiodarone, an acute inferolateral myocardial infarction (ST segment elevation in L 2, L3, AVF, and V5-V6) with marked ST segment depression in V1 to V3 was observed (Figure 3).
{kind=link}
{kind=link}
{kind=link}
Angiography:
1) LM normal
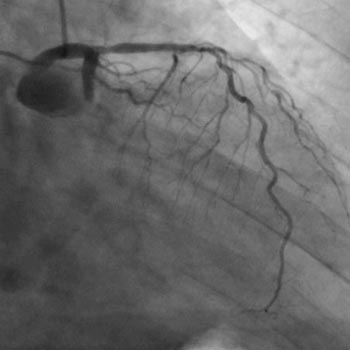
2) LAD 50% mid vessel stenosis (Figure 4)
3) LCX 100% occluded
4) RCA multiple 50% stenoses and a long segment 90% PDA stenosis (Figure 5)
{kind=link}
{kind=link}
Procedure:
The left coronary artery was engaged by a 6Fr 3.5 XBU guiding catheter, and a CrossIt 100 guidewire was negotiated across the total occlusion (Figure 6). After manual thrombo suction by a 6Fr Export catheter and intracoronary tirofiban ( 25 mcg/Kg) bolus injection, a tight residual stenosis was seen. A 2.75x12mm sirolimus eluting stent was deployed at 18atm. Brisk antegrade TIMI 3 flow was achieved with no residual stenosis (Figure 7).
{kind=link}
{kind=link}
Conclusion:
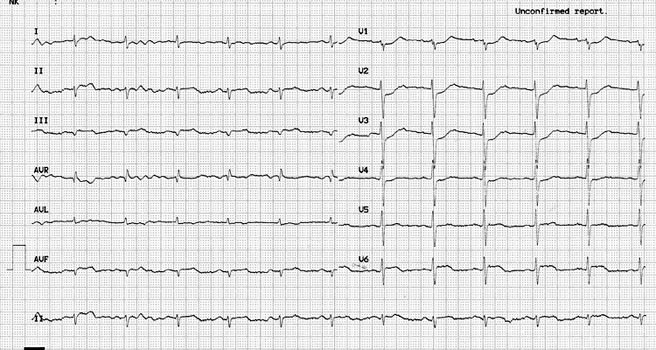
There was rapid disappearance of chest pain and near complete resolution of ST segment elevation in the inferolateral leads suggesting good myocardial perfusion (Figure 8). 2D echocardiogram demonstrated inferior wall hypokinesia with global ejection fraction of 50%. The patient was maintained on adequate oxygenation, and his serum potassium and magnesium levels were within normal limits. The patient was discharged 3 days post-admission on oral amiodarone . He did not receive any IV infusion of amiodarone.
{kind=link}
Comments:
Primary sustained ventricular tachycardia is usually polymorphic and carries worse in hospital prognosis than patients without ventricular tachycardia. However, there is no increased recurrence or sudden death at one year follow up. The patient did not receive an ICD as patients surviving sustained primary VT have similar survival as patients who do not have primary VT. Moreover, this patient had an LV ejection fraction of 50% immediately post-PCI. Prompt revascularization by salvaging substantial myocardium and preventing recurrent ischemia aids in rectifying the electrical instability that accompanies acute MI.
Conflict of Interest:
None