DOI: 10.1056/NEJMoa2007621
Drugs used in treatment of hypertension, heart failure or diabetes do not increase risk of higher rate of infection, severity of dies or death in patients with Covid-19. Covid -19 disease is caused when SARS-CoV-2 ( a beta coronavirus) enters your body via receptors called ACE 2 (angiotensin converting enzyme 2). At the beginning of the pandemic it was theorised that popular and effective classes of medicines often used to treat hypertension ,heart failure or diabetes , would be detrimental because they increase the ACE-2 receptor. The logic was single , a lot of hypertensives and patients with heart failure were falling down dead with Covid-19, so the usage of these drugs may explain increased mortality. The drugs are named angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blocker (ARB).
Examples of the ACEI group of medicines are ramipril, lisinopril, trandalopril, captopril…….so they can also be called the “prils.”. The angiotensin recep[tor blockers are losartan, telimisartan, valsartan……..also termed the “sartans.”. Randomised rials done over decades have confirmed efficacy and safety of these medicines in treatment of hypertension and heart failure. SARS-CoV-2 , the coronavirus, penetrates human cell by using the spikes attached to its surface on to the ACE2 receptors present in abundance in the lungs, heart, intestines , and kidney. It was no surprise that Whatsapp messages were spreading like wildfire regarding these medicines.
“Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection?” This was the title of this scientific letter written to The Lancet on March 11, 2020 (Published OnlineMarch 11, 2020 https://doi.org/10.1016/ S2213-2600(20)30116-8). The authors of the letter went on “ suggest that patients with cardiac diseases, hypertension, or diabetes, who are treated with ACE2- increasing drugs, are at higher risk for severe COVID-19 infection and, therefore, should be monitored for ACE2-modulating medications, such as ACE inhibitors or ARBs’. A conundrum was treated for clinicians , because millions of patents were at stake. Do we continue with an ACEI or ARB or not was the burning question clinicians were asking amongst themselves ?
The picture is clearer now with 3 good, albeit, observational papers recently published. A large study included 8910 patients in 11 countries across 3 continents. All patients had been hospitalised. By applying statistics (multivariate logistic-regression analysis) they found out that age >65 years, coronary artery disease, heart failure, history of arrhythmia, chronic obstructive lung disease and current smoking were associated with raised risk of death. Females had a lesser risk. Importantly, both ACEI and ARB were not associated with increased risk.
An Italian study from the region of Lombardy similarly showed no increased risk with ACEI or ARB’s in confirmed cases of 6272 Covid-19 patients when compared with more than 30,000 controls having similar sex, age and place of residence. Once again logistic-regression multivariate analysis failed to show increased incidence of Coivid-19. Also there was no increased risk associated with these drugs in severely affected patients or in patients who died.
DOI: 10.1056/NEJMoa2008975
The third study analysed data from health records of 12, 594 patients; of these almost 6000 patients were founds to be infected. More than 1000 had severe infection, defined as admission to intensive care, ventilation or death. The researchers did not find association for any of the analysed drugs for a positive test to severe illness.
All 3 studies negate the theory that ACEI or ARB is associated with risk of SARS-CoV-2 infection , severity of illness or risk of death. There was a hint in one studies that there was in fact a lower risk of in hospital death with use if ACEI or statins, but this cannot be taken for granted as this was an observational trial. Every professional scientific society has advised ACEI or ARB should not be stopped due to concern of increased susceptibility or severity of Covid-19 infection.There is also no increased risk with other classes of medicines such as beta-blockers, thiazide diuretics and calcium channel blockers. Hence despite the theory that ACEI’s or ARBS’s could increase levels of the ACE2 proteins that happen to be the entry point for SARS-CoV-2 into human cell, there is no increased risk of Covid-19 infection or death by it.
Lancet Respir Med 2020
Published Online
May 13, 2020 https://doi.org/10.1016/ S2213-2600(20)30224-1
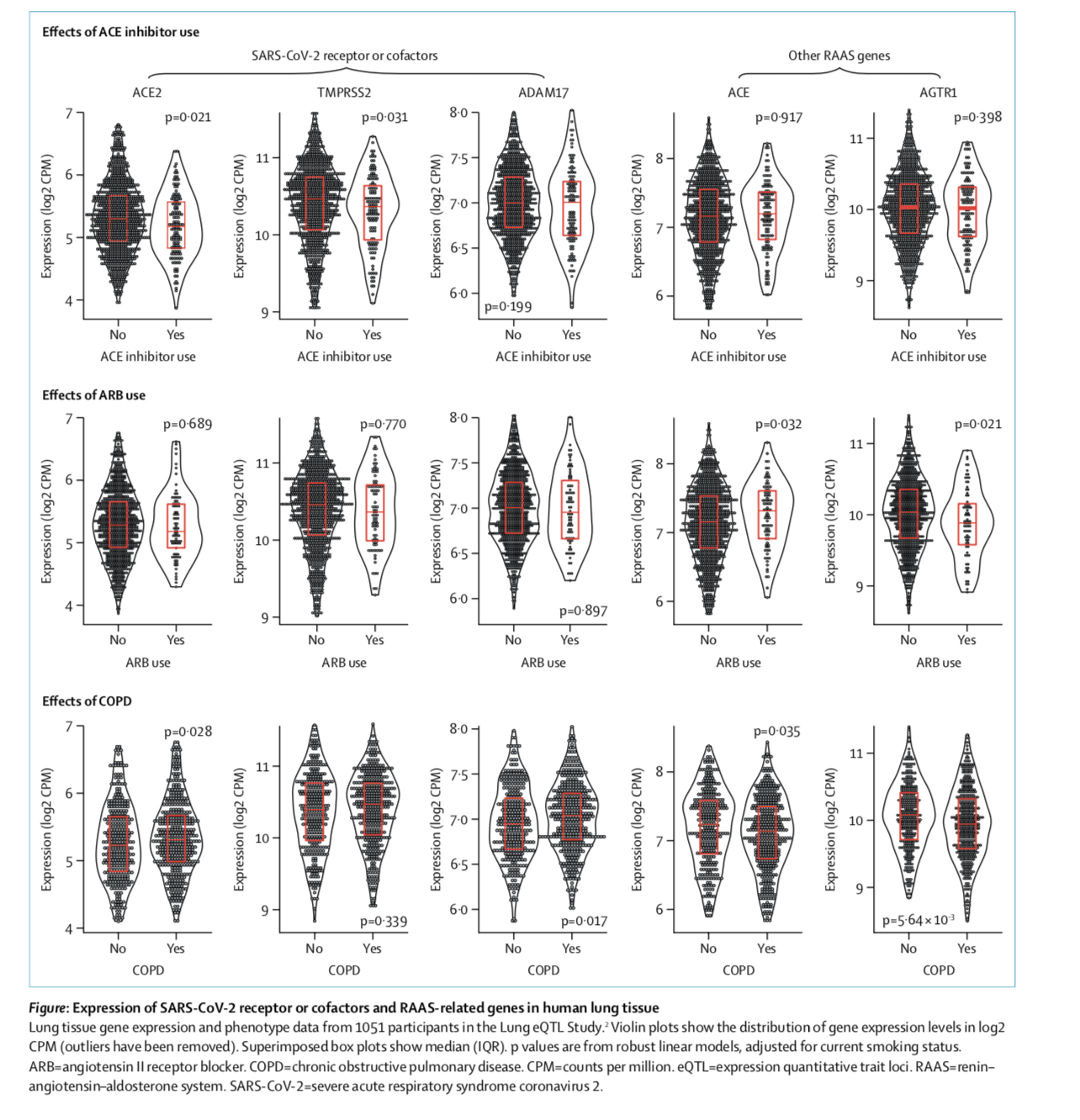
A recent letter in the Lancet describes experimental evidence that ACEI actually down regulates the ACE2 receptors in lung tissue. “It is possible that long-term ACEI use downregulates lung ACE2 expression by reducing substrate (ie, angiotensin II) availability, which might also explain why no effect of ARBs was seen. In theory, ACE2 down regulation might reduce the risk of SARS-CoV-2 infection because of reduced virus receptor availability.” But animal studies that reduced ACE2 can increase acute lung injury. The clinical significance of effect of ACEI on the ACE 2 receptor however remains unclear.
The message is simple , do NOT stop your blood pressure pill, lock down or no lock down.