If you can’t solve the problem, you are not employing evidence.
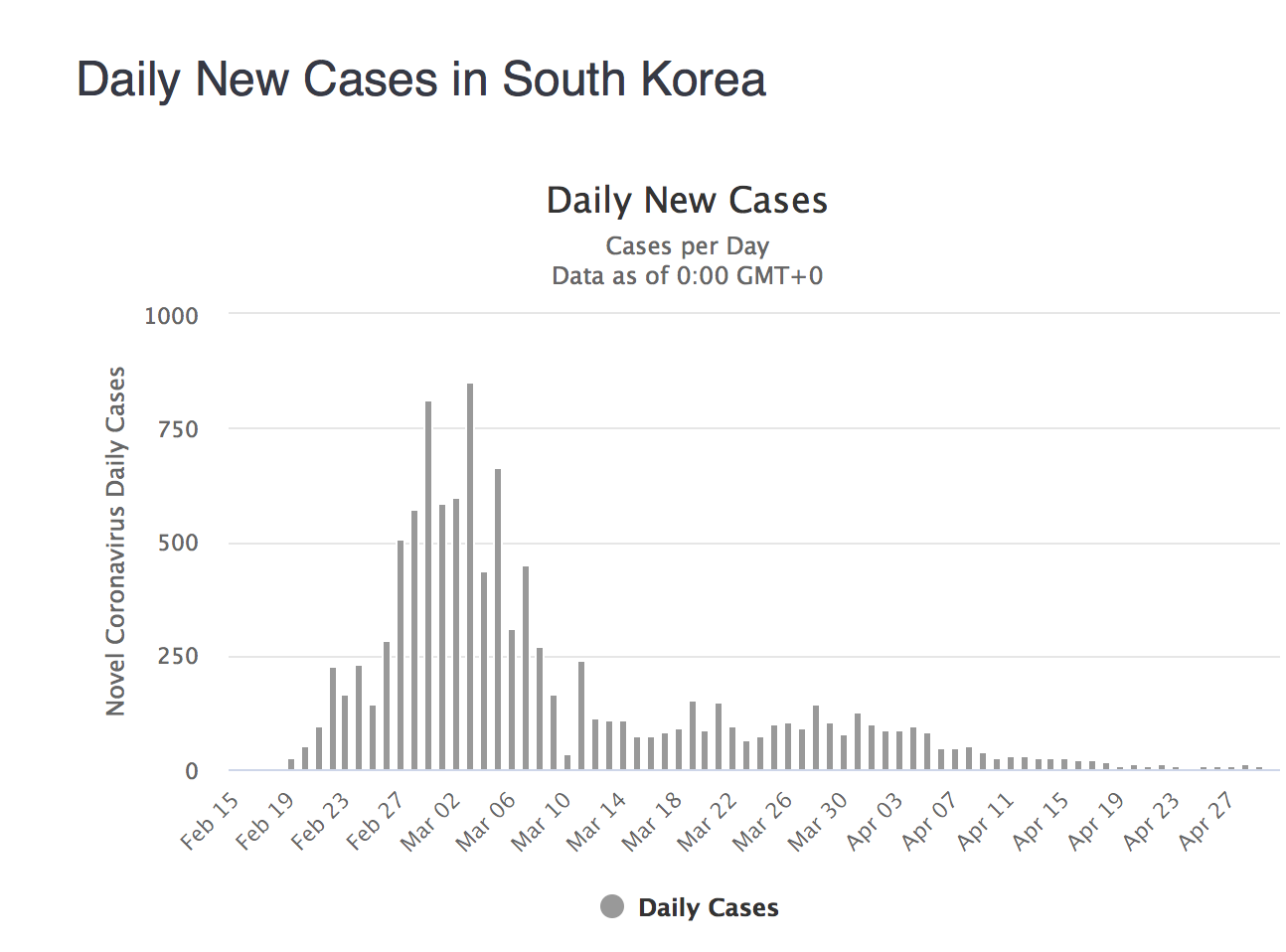
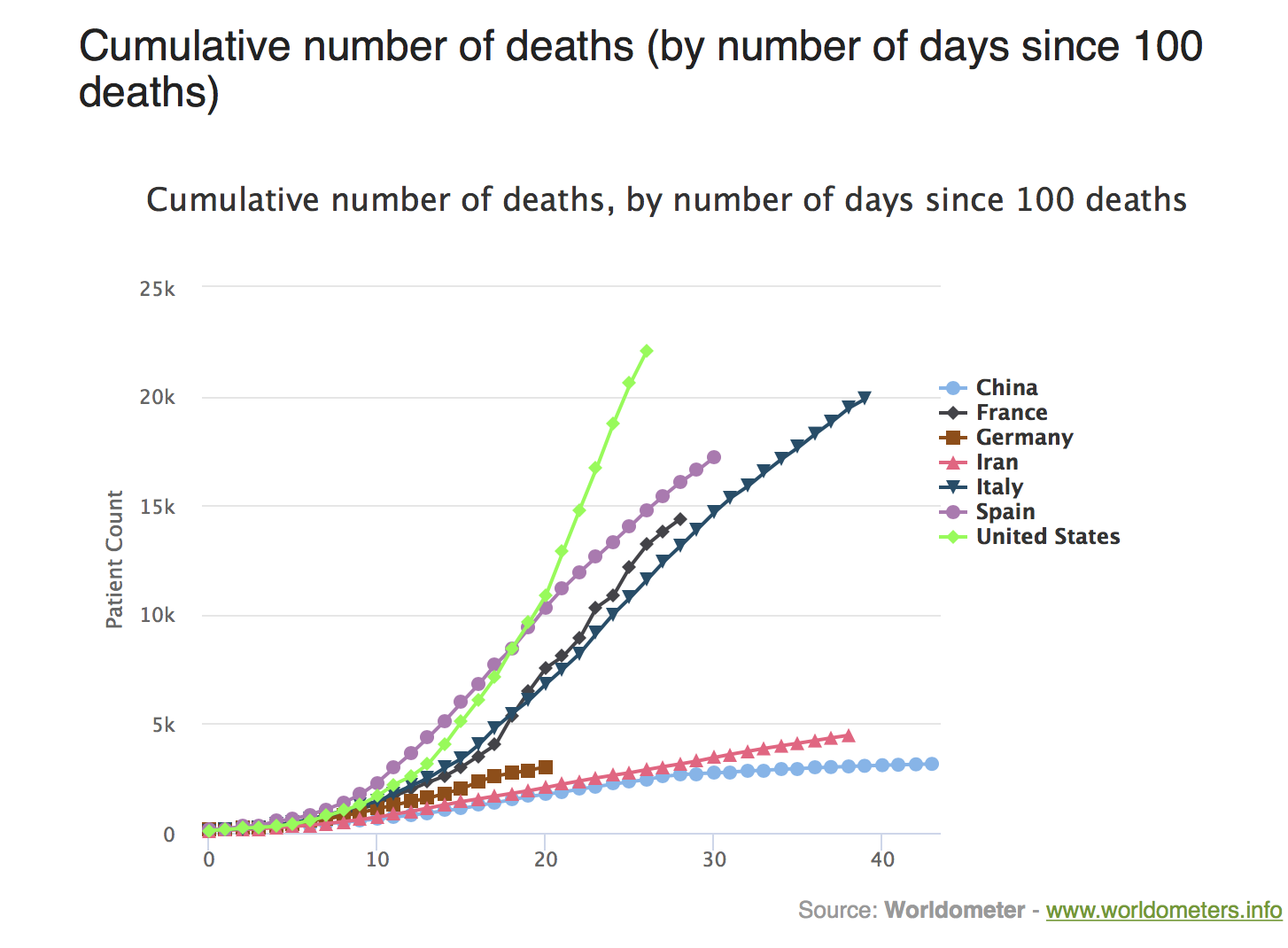
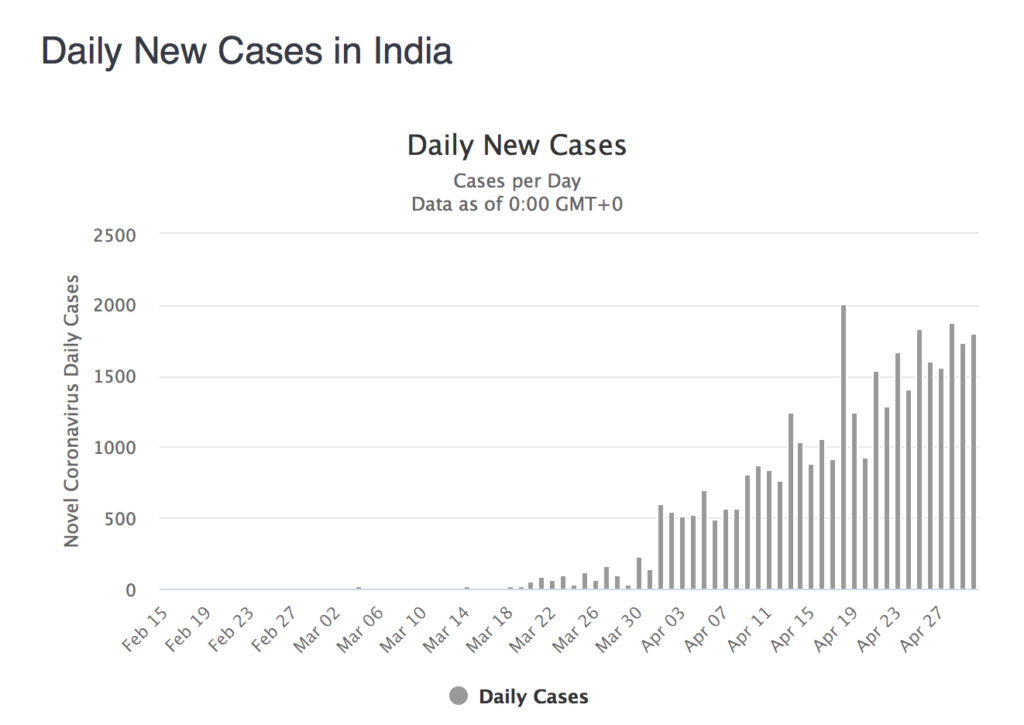
A lockdown CANNOT be imposed on a whim or a gut feeling. Crucially it should NEVER be imposed to garner approval ratings. There has to be a science behind it; the decision must be evidence based, not a reflection of a house constructed from sand. The lock down in India is laughable. It was imposed around the 25th of March. As per the WHO, there were a total of 434 cases that day, with a total of 9 deaths. Italy had 63927 cases with 6077 deaths, and the USA had 42,164 cases and 571 deaths. We now have more than 33000 cases with 1074 deaths, around 67 died yesterday. The lock down has obviously not worked one bit. The timing of the lockdown was too premature, draconian measures were imposed much before cases had begun to mount. No attempt was made by the government or the media to assure the public that all data on Covid-19 pointed to more than 80% people developing mild or no symptoms. The majority of people would simply shrug off the virus with absolutely no harm to themselves, especially if they were young (as most Indians are) or had no underlying disease.The number of cases keep rising every day for the simile reason that more people are being tested now than before. Mercifully the number of deaths are still in double figures. In previous years more than 20,000 Indians died in one day, because of a variety of reasons. This is not the time to discuss them but stay focussed on what is happening right under our noses. Millions of people have been displaced, lakhs of businesses are shuttered, all schools closed , restaurants and hotels shut, and manifestly millions without jobs or any means of sustenance. The poor have been hit like never before and before they realise it , the middle class will begin to crumble. Crores of children are corralled with unimaginable psychological adverse effects, domestic and child abuse that largely go unreported must be substantially elevated. These matters are well known to you. But the timing of a lock down is hardly known to the lay public or even most doctors. It is the job of public health doctors or epidemiologists. Most public health doctors worth their salt will endorse the fact that a lock down if needed must coincide with the peak incidence of cases; it should NEVER be too early or too late. It must be put in place at peak infection. The graphic provided clearly shows that despite the lock down cases in India have shown no decline. There has been a steady increase in number of cases since mid March; what could be the reason for this? The treason is simple, faulty timing of the lockdown.
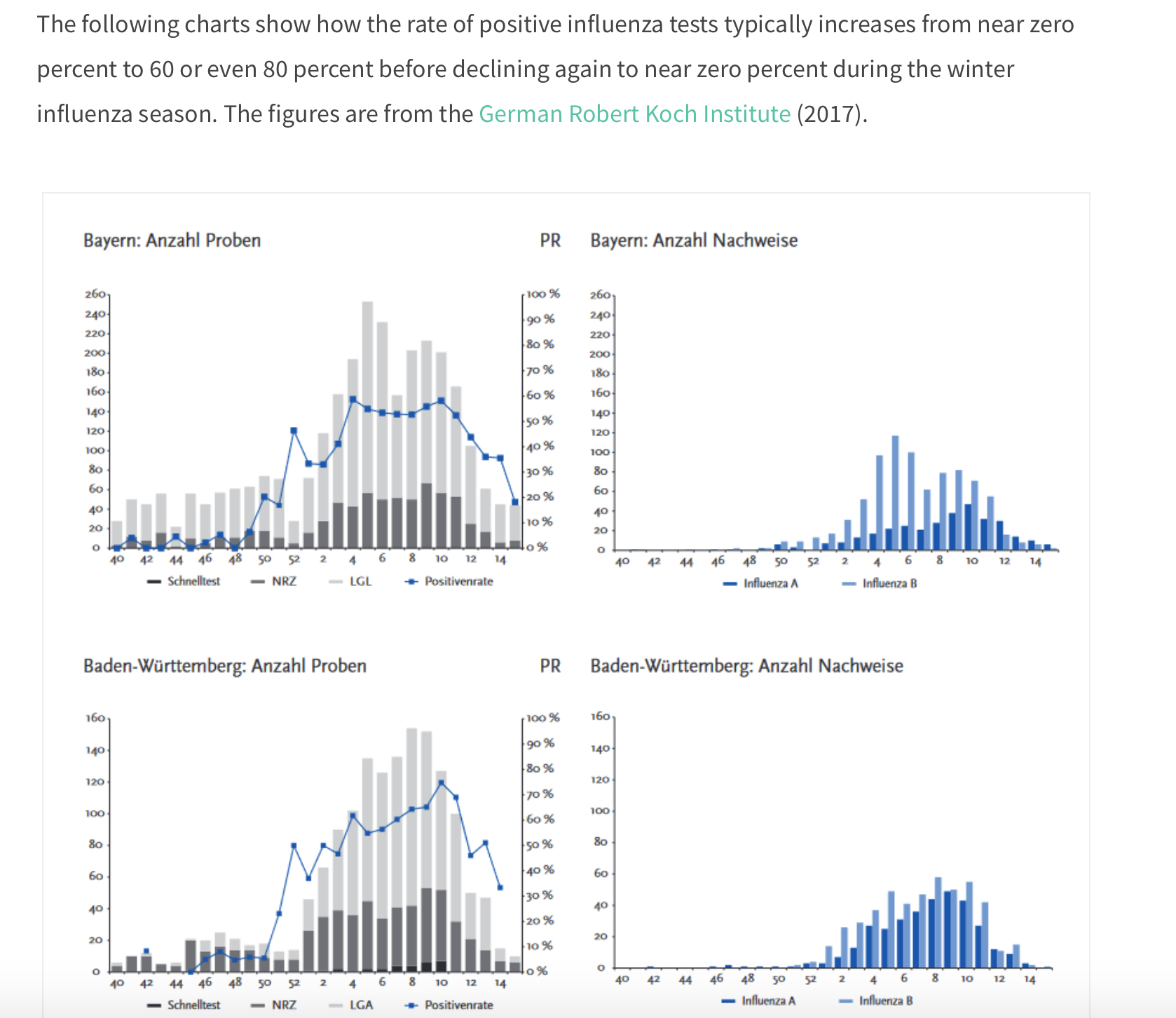
SARS-Cov-2 is basically a respiratory virus, evolved from nature. Even if man made as some conspiracy theorists may imply it is near identical to SARS-Cov-1 and other corona viruses. It is also similar tom other viruses that affect the respiratory system , including the flu virus. Every respiratory virus, particularly the flu virus, has a pattern, it emerges in winter and after infection people for 6-8 weeks makes a retreat. In the process the flu virus manages to kill 30000 to 60000 people in the USA alone, and millions worldwide, without much hue and cry.
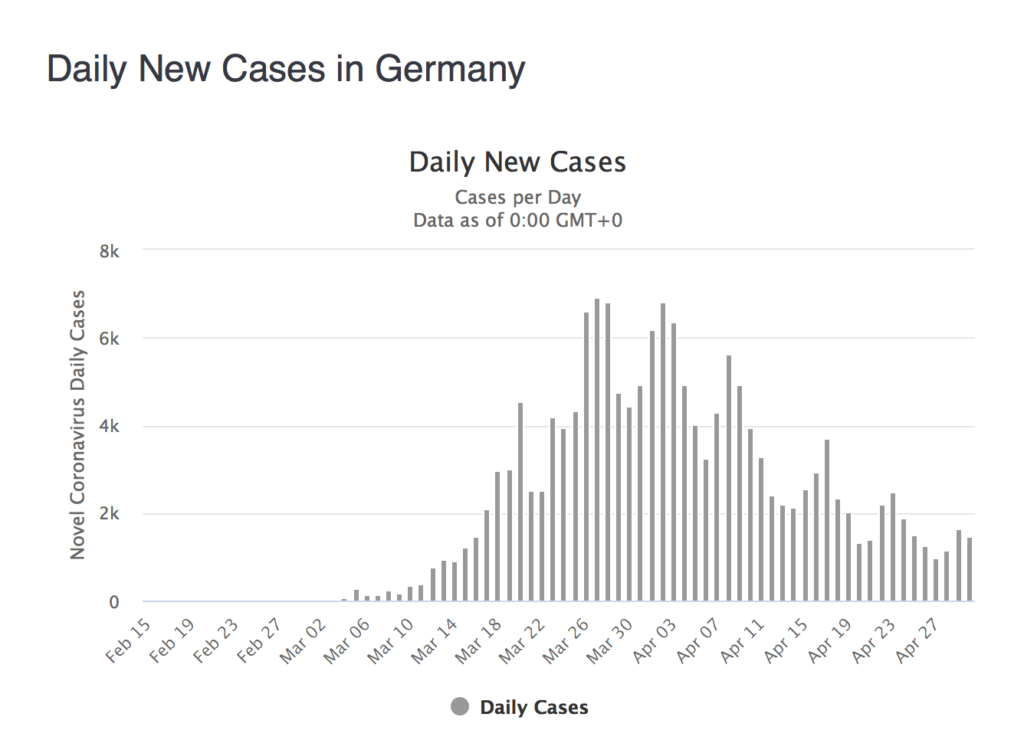
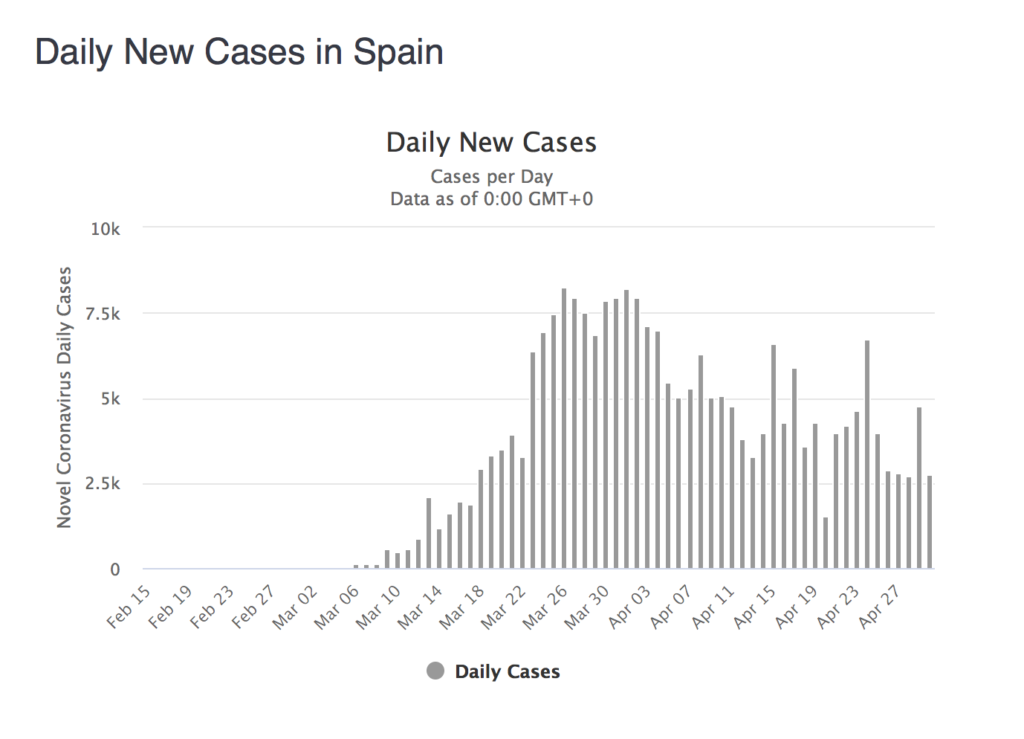
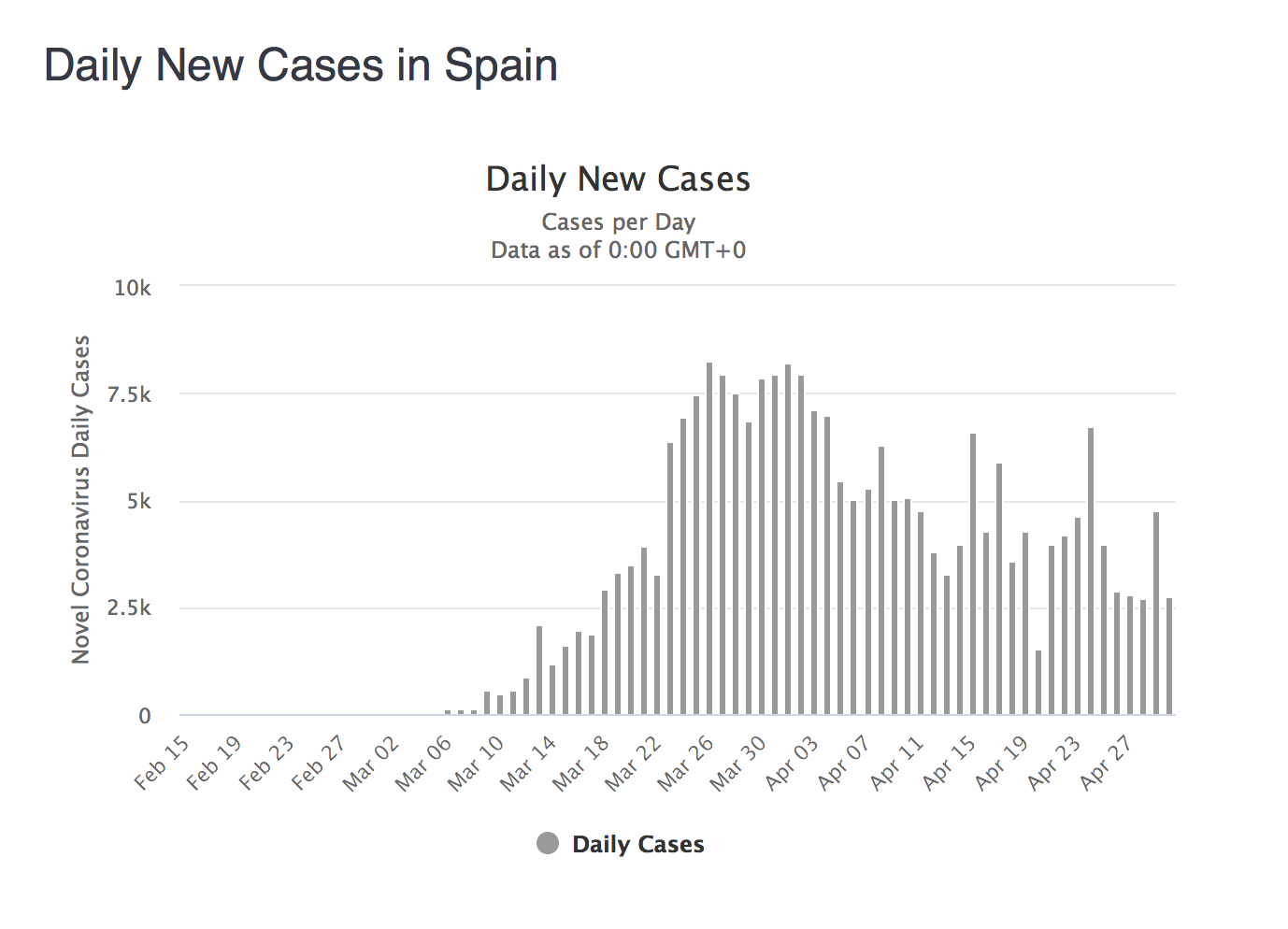
Covid -19 has played havoc in Spain and Italy but as expected the number of new cases are declining (seen in the graphs), the graph will be the same for almost all countries. A rapid increase in new cases and then fall in numbers over 4-6 weeks. This has been the natural history of flu as can be seen in the graph from Germany. But the moment a lock down is imposed you interfere with the natural history of the disease. The curve is simply flattened at most, meaning that cases/.deaths will take place but will be spaced out or delayed. The logic behind flattening the curve was to buy time to improve logistics in hospitals , get more beds and ventilators and PPE’s. And also to ramp up the ability to test for the virus and check for past infection (antibody tests).

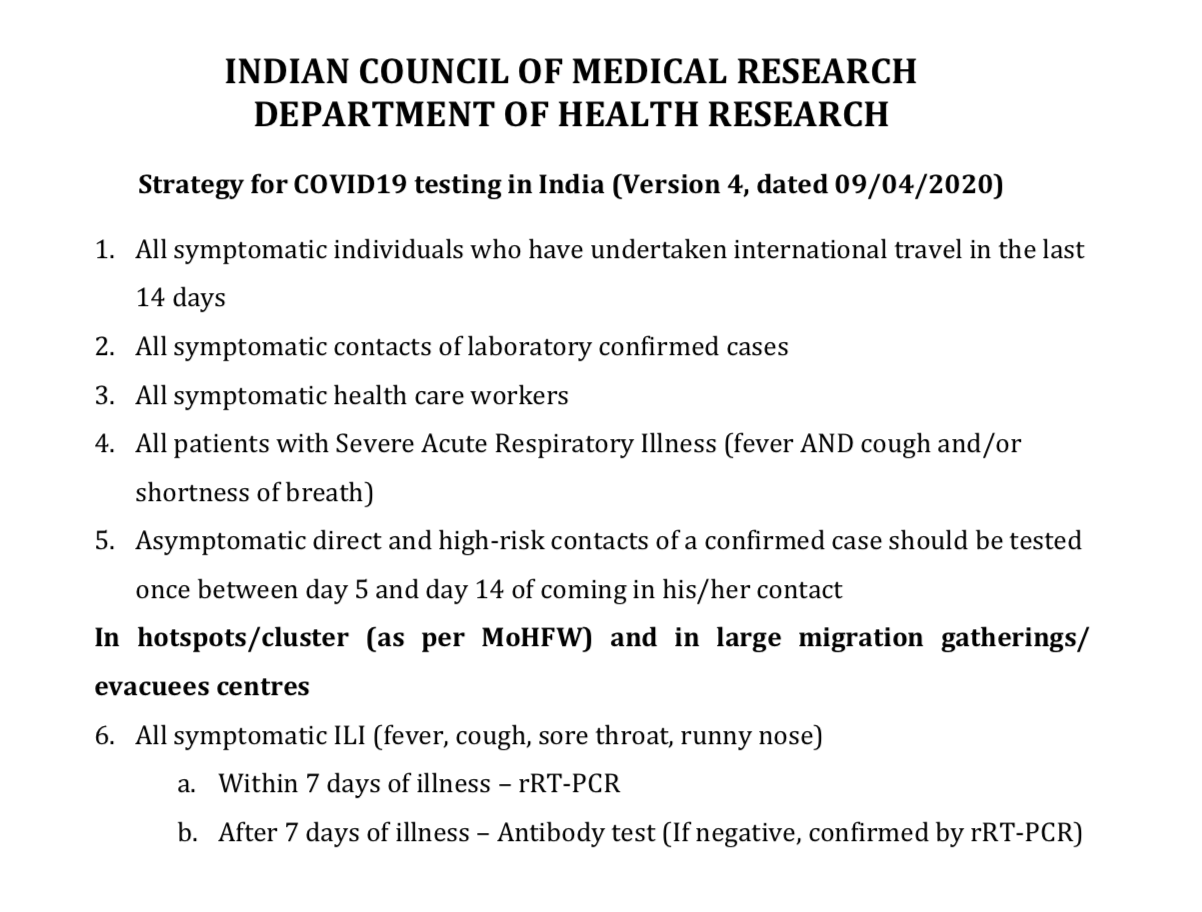
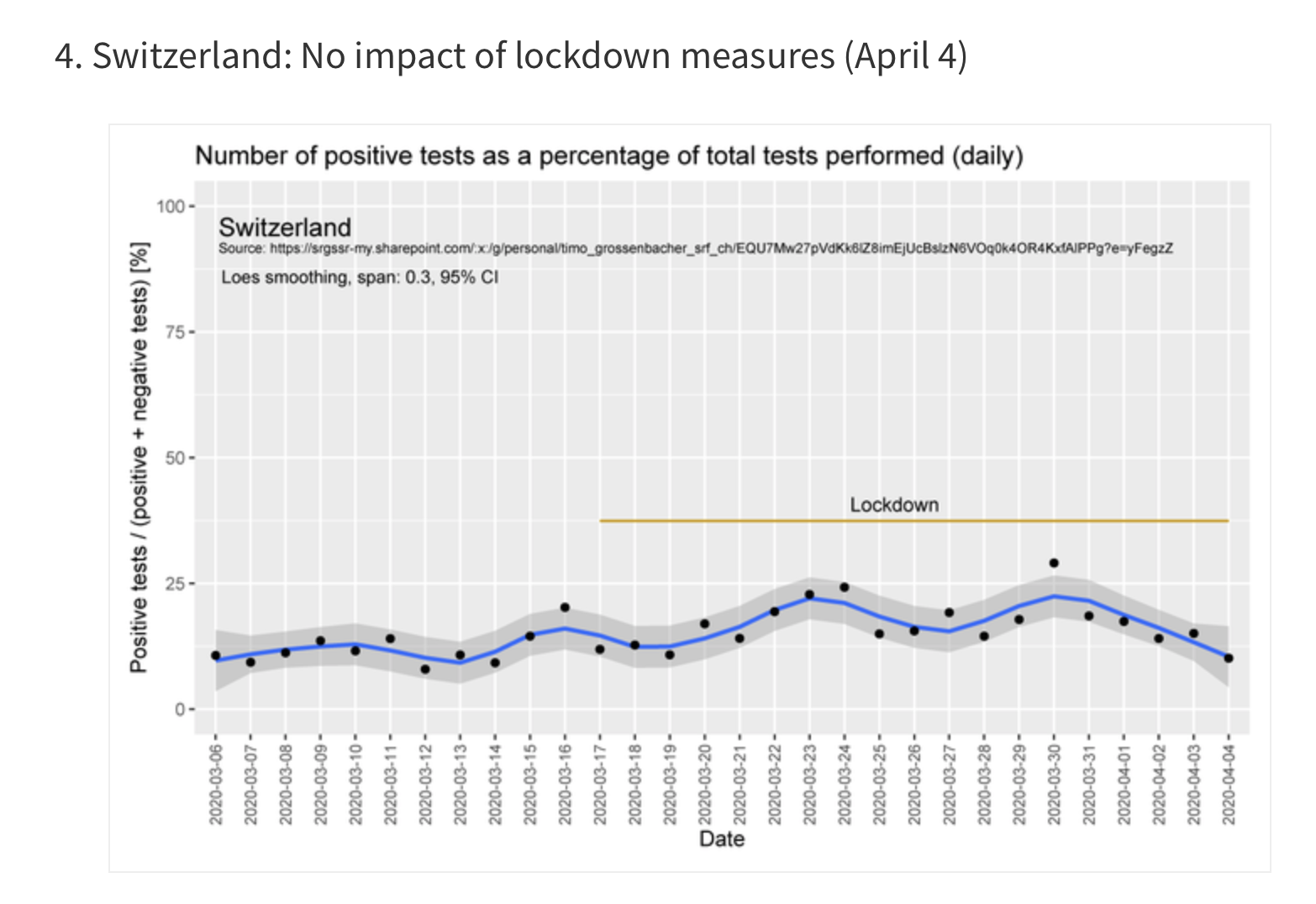
The lockdown has done little to the number of new cases detected in Switzerland.. The situation is more or less the same in India. Switzerland is on the brink of unshackling , while India keeps extending it despite no advantage. The proportion of new cases detected in India is considerably less than other countries; where it ranges from 5 to 25%.In India it hovers around 4% only.

The situation however was completely different in India, the cases have been remarkably few and deaths fewer. The main reasons are 2; a younger population cohort and much higher temperatures than Wuhan, Europe and the US. Let the so called experts say whatever they want, a 35 C plus temperature will paralyse this virus. The small number of cases is ample evidence. Some may argue that the lockdown has been our great saviour. Not true. Because the new cases keep coming each day despite the most draconian lockdown on the planet, yet they are few. Most hospitals are lying empty with health workers twiddling their thumbs. The corporates have already announced significant reduction in salaries of doctors.
The ministry of health predictably has been found wanting on every front. The mandarins and their advisors seem to come from another planet or are just confused. A neighbouring country announces the arrival of a new respiratory virus on January 10th, and we do not still have a validated antibody test with us on May 1st ! So much for our preparedness or reflexes. This is a cruel joke that a nation that attempts at an unmanned landing on the moon , does not have the scientific intellect to set up an antibody test over 4 long months. Worse no one seems to care, just about no one. Even the medical fraternity, which should have been screaming for serological testing for themselves have drowned itself in deafening silence.
It is imperative that we know the incidence of infection. For example they did in 3300 people in Santa Calra, to find that 2.5-4% people had past infection or antibodies. The study was done by Stanford University if you like credentials. The simple math is that around 50000 to 85000 people in Santa Clara county have been infected, but only 1000 people had tested positive by PCR. The conclusion, and a correct conclusion, is that the true prevalence of Covid 19 is 50 to 85 times more than the PCR estimate. Use the math in India, around 3600 cases and 1200 deaths, a crude mortality rate of 3.3%, but if we extrapolate from the Santa Clara data mortality is less than 0.04% by Covid-19. Instead of telling the true death ratio, the media keeps banging non stop on the dangers of this virus. The propaganda has been terrific because I am sure if people were asked for loosening a significant number would clamour that it be kept on for 6-8 weeks more. People have become paralysed by fear, they are scared out of their minds. It will take a miracle to mitigate their apprehension or rather terror. Most doctors are so scared witless that they prefer staying not 6 but 12 feet away from a patient. These are remarkable times. The politician and his Babu in the blink of an eye are prepared to seal a hospital if a couple of cases are discovered in a hospital. Sealing a hospital on finding a Cover -19 case, which kills less than 0.05% affected people is more than absurd, it is scary. Albert Camus wrote of bad and good people in his fabulous book “The Plague”, but he too could never have imagined that the nation of the Mahatma would go around sealing hospitals if a case was spotted within them. Where else would you expect to find this virus if not in hospitals ? People go to hospitals for treatment but now you scare the hell out of them by sealing hospitals. No wonder thousands of patients are petrified of visiting a hospital even as they suffer chest pains or paralysis. Mark my words, there will be far more deaths die to heart attacks, cancers and strokes in the next 2-4 years, than Covid-19. A bizarre and impossible situation has been created in this country. How many know that Gandhiji actually treated patients of pneumonic plague in Johannesburg. Pneumonic plague has always been a killer, but Gandhiji had the guts in 1904 to actually try to treat the patients. The leadership today is limited to delivering messages on TV and Twitter. This is a fact, I do not know which leader has mingled with the people (albeit from the prescribed distance) or visited a single hospital. Instead it has been the usual vacuous soundbites with minuscule substance, and even lesser (if possible) reassurance. This virus has no respect for caste, creed, religion or political affiliation. It demands that we shed our intellectual laziness and get to know the truth in order to tackle it. But if we do not it certainly will not mind.
New York too tested 3000 people for antibodies to find that 14% had been infected, in fact 21% of New York City inhabitants were infected. The implication again was that almost 27 lakh people had got infected , the good news was that armed with this knowledge the Governor Andrew Cuomo could publicly declare an infection fatality rate of 0.5%. The numbers should be tempered with the knowledge that numerous patients got treated by ventilators that proved detrimental. Why then in Gods name are people so scared of this virus? So terrified that they have gone to the extent of sealing Delhi from both NOIDA and Haryana. Apparently Haryana police has dug up roads at the border as if they anticipate a tank brigade to attack them. It is a ludicrous situation. Laughable. I was compelled to to do 2 PTCA procedures yesterday. Both patients we’re hanging by a thread. The procedure by any standards was life saving in both of them. We knew the first patient was Covid-19 negative because he had been tested. The second patient was a post CABG man who entered the emergency room with sustained ventricular tachycardia and BP of 70 mm Hg systolic. He needed a 20 joule DC stock for reversion before he was hastily wheeled to the Cath lab. He had had severe chest pain preceding the VT, and so the procedure was absolutely essential. Both patients had successful procedures and wished to be discharges as soon as possible, that is today. A patient expects the doctor who has done a major procedure on him to examine him before discharge. So it was with these 2. But alas it could not be done. To my utter horror I was stopped at the border this morning on my way to hospital. The hospital falls in Dwarka, Delhi whilst I currently reside technically in Haryana. So thats it folks; I did not bother bro treason with the rotund pot bellied policeman, I knew it was a waste of time. The man had orders from “above.” The situation is just hilarious. A pandemic has gripped the planet. All agree an epidemic unfolds in this country, but the high command is not prepared to permit doctors from treating patients. George Orwell would have never thought of this one. In fact this is not a “new normal,” this is a “unique normal.”
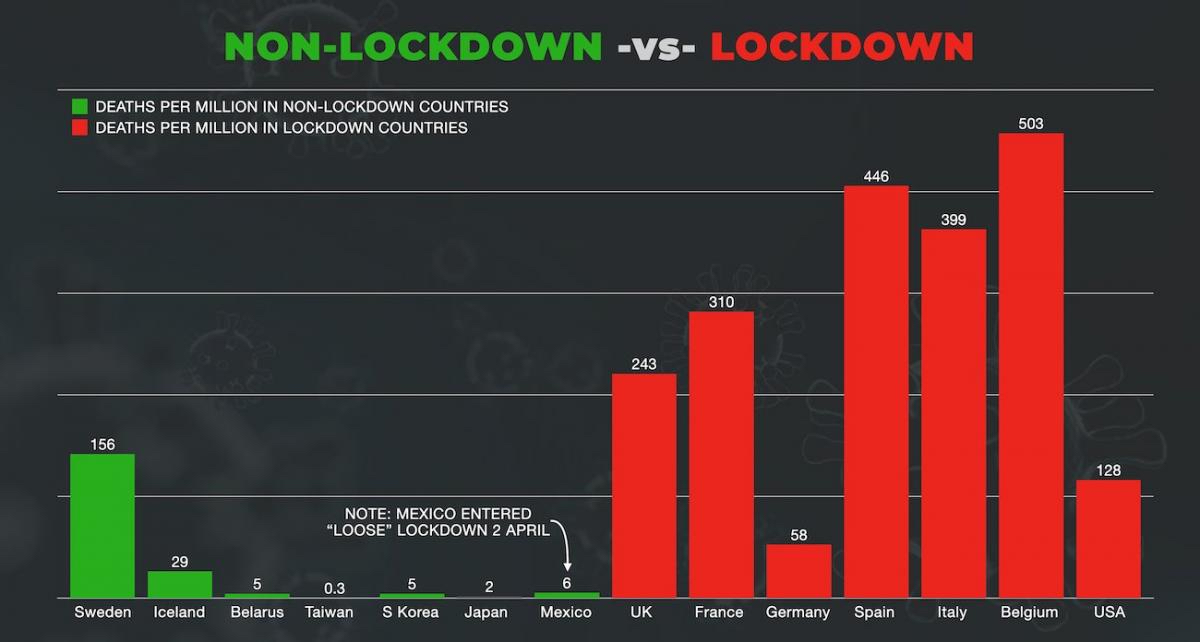
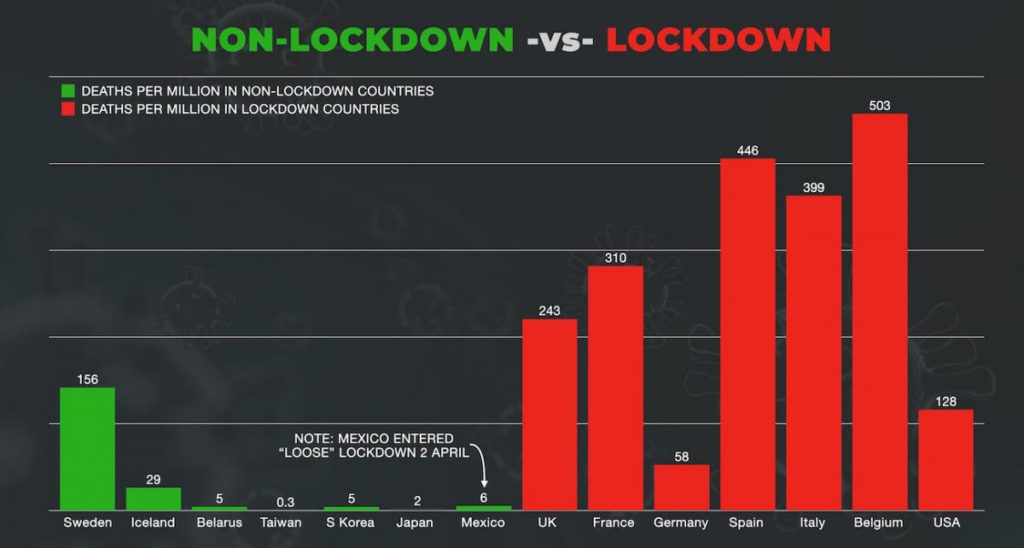
Sweden is not under lockdown. It never went under lockdown. Schools and restaurants are open. People have been advised to maintain distance amongst themselves and apply common sense. They anticipate herd immunity by the next fortnight. Moreover their death rate is substantially lower than other European countries. It is more than their neighbours who are under lockdown but expect the figures to level off by the time the season is over. There is grudging admiration for the Sweden model; despite orchestrated critiques thrown in influential media sources. Mercifully the Swedes did not buy the “Ferguson from Imperial College “ fame that 2 million would die in the US and 50000 in Britain if a lockdown was not imposed. Remarkably Ferguson did not publish a peer reviewed paper any where. Moreover Imperial college does not even have a pre reviewed paper anywhere. They just have a document that forced the Brits to make a U turn. The same Ferguson then gave testimony before parliament that deaths would be around 20000 and two thirds of these would be deaths in the normal course off events. It must be kept in mind that almost 50% of deaths in Europe including Sweden have been in old age homes. Ironically the people for whose protection the lockdown was imposed in the first place turned out sadly to be the ones that got most neglected. Sweden has conceded to this sad state of affairs and is making amends.
We have faltered at every stage of this epidemic. We never got PCR testing done on time, we even today do not have a validated serology test, we have absolutely no randomised data on any intervention attempted during this pandemic, an ill timed lockdown is inflicted without any scientific evidence, we have no idea when was the peak of new cases, even today we do not know the virus genome, and crucially we have absolutely no clue of the infection rate. We all wait with bated breath for a vaccine to materialise in the next 6 to 18 months, in the meantime we are the classic deer in the headlights. It is imperative that we read up on this virus, attain some clarity while shedding off the trepidation. It is not enough to watch TV all day, especially not the health ministry sermons, it is time to realise that sealing hospitals, sealing borders and extending this lockdown indiscriminately will not prevent infection in the slightest way. A man of 42 years was turned back from a hospital in Delhi yesterday for a Ciovid-19 test. He had gone to hospital for chest pain, he died in his way back. Maybe he has gone to a better place, most probably he has. Sealing borders and hospitals is the trend today. Patients should expect to be treated by chaps who present glitzy pandemic models or mandarins of the health ministry. You declare a pandemic, create coloured zones, constantly go on that the virus lurks in front , behind and around you, continuously remind the average man that he is a sitting duck if he gets infected, and then merrily prevent a doctor from going to the hospital. Incredible India. Enforcing a lockdown without a shred of evidence is easy, but what parameters will you apply to lift it?
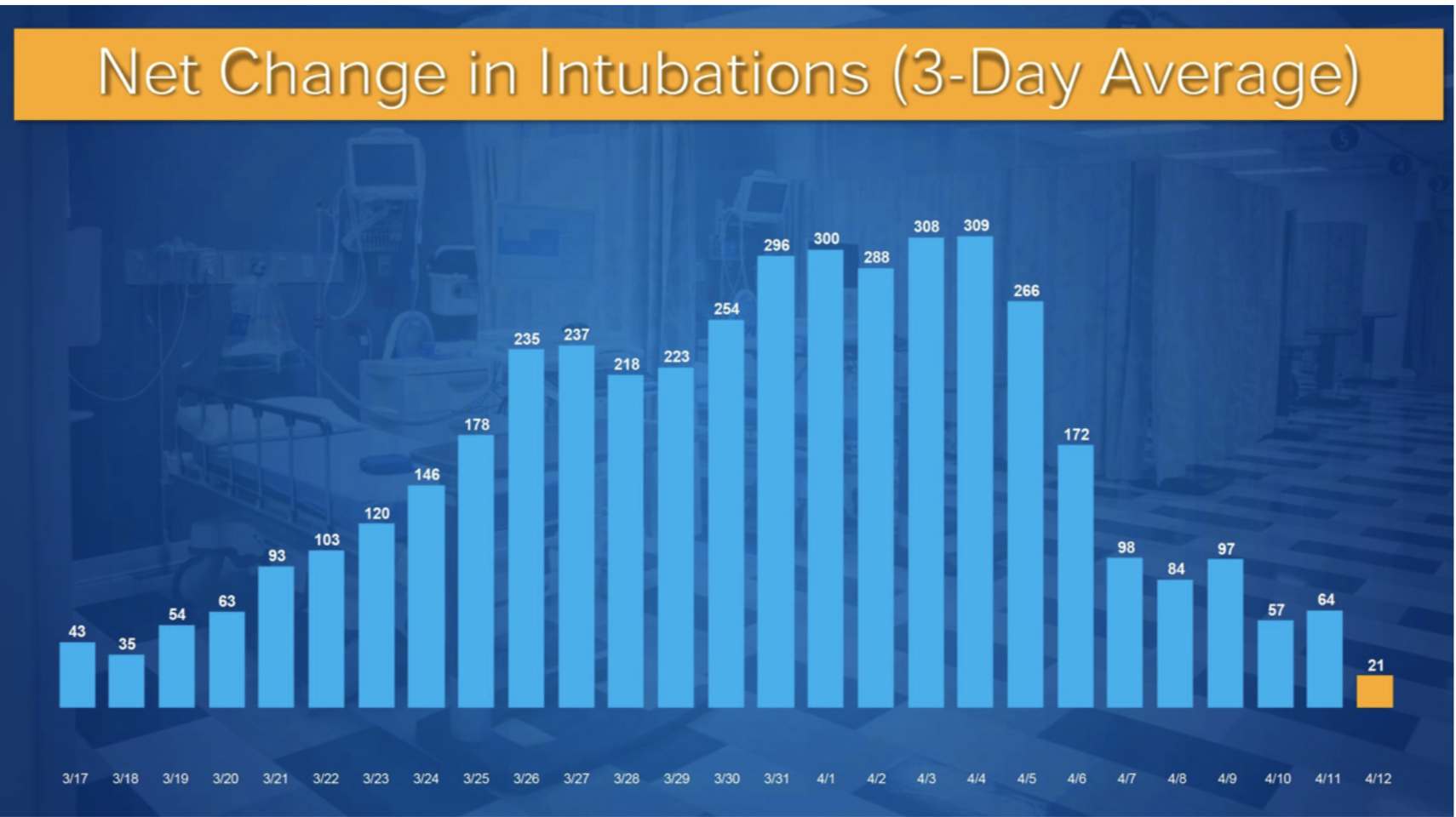
As of now there has been no impact on the curve, as was expected. Each new day brings more cases. If the lockdown is lifted the virus will come roaring back because most people would not have developed immunity against it, while confined in their homes. The elderly will continue to be vulnerable. The misery that has been inflicted on crores of people is compounded by the fact that a staggering amount of time, money and lives have been wasted. amid an officially declared national medical emergency preventing a doctor from crossing the Delhi Gurugram/NOIDA border is not only bizarre but plain idiocy. The obsequious babu in his zest for lockdowns is totally oblivious of the fact that there are hundreds of other serious ailments apart from Covid-19 demanding both attention and treatment.