By Deepak Natarajan
Monday, May 11, 2009
Operator(s):
Deepak Natarajan MD, DM
Affiliation:
Indraprastha Apollo Hospitals,New Delhi
Facility:
Department of Cardiology, Indraprastha Apollo Hospitals, New Delhi, India
History:
A 75 year-old hypertensive male with left lung upper lobe resection for carcinoma in 1997 and PCI with stenting of his right coronary artery (RCA) with a bare metal stent (BMS) in 2002 was admitted for unstable angina and shortness of breath for the past 5-6 days. His ECG revealed right bundle branch block with ischemic ST segment changes. The troponin-I was significantly raised. The 2-D echocardiogram demonstrated mild apical left ventricular (LV) hypokinesia with a global LV ejection fraction of 54%.
Angiography:
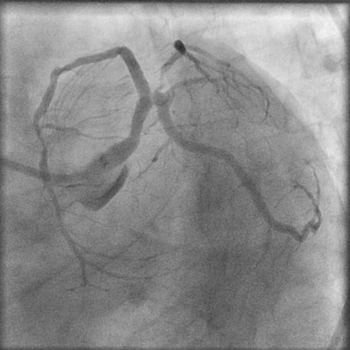
- LM: distal 60% eccentric stenosis



- LAD: ostial 90% stenosis with additional 70% proximal stenosis.
- LCX: no disease
- RCA: 80-90% BMS restenosis

Procedure:
The RCA was engaged first with a 6Fr JR guiding catheter, and a Hi-Torque Whisper MS guidewire was negotiated through the in-stent restenotic lesion and sequential balloon angioplasty attempted with 1.5x12mm,2x12mm,2.5x10mm, and finally 3.5x15mm balloons inflated to 14atm  achieving TIMI 3 flow with minimal residual stenosis
achieving TIMI 3 flow with minimal residual stenosis 
The left coronary artery was next engaged with a 7Fr EBU guiding catheter with a 3.5cms curve, and a Whisper guidewire placed into the distal LAD artery while an ATW 0.014 inch floppy guidewire was positioned in the LCX. The LAD stenoses were predilated sequentially with 2x12mm and 2.5x12mm balloons. A 3.5x32mm TAXCOR paclitaxel-eluting stent (PES) was deployed from the LMCA to the proximal LAD across the LCX
A 3.5x32mm TAXCOR paclitaxel-eluting stent (PES) was deployed from the LMCA to the proximal LAD across the LCX 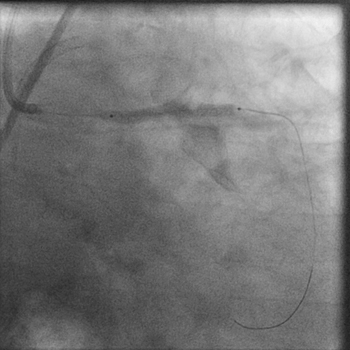 initially at 12 atm. Subsequently the LCX guidewire was removed, and the PES further inflated to 18atm. A 3.5x10mm noncompliant balloon was next used for post-dilation at 24atm.
initially at 12 atm. Subsequently the LCX guidewire was removed, and the PES further inflated to 18atm. A 3.5x10mm noncompliant balloon was next used for post-dilation at 24atm. 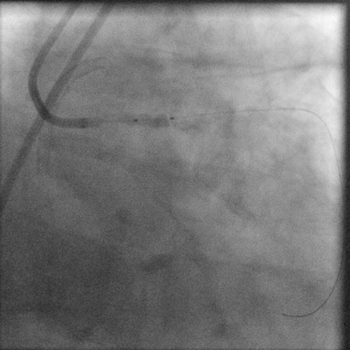 TIMI 3 flow was obtained in the left coronary arterial system with no residual stenosis or dissection. There was absolutely no jailing of the LCX and therefore no kissing balloon was performed.
TIMI 3 flow was obtained in the left coronary arterial system with no residual stenosis or dissection. There was absolutely no jailing of the LCX and therefore no kissing balloon was performed. 
Conclusion:
His further stay in the hospital was uneventful, and he was discharged after 2 days on triple anti-platelet therapy consisting of aspirin, clopidogrel, and cilostazol.
Comments:
Percutaneous coronary intervention in unprotected LMCA lesions with drug-eluting stents is emerging as an alternative to CABG. The large SYNTAX randomized study comparing PCI with CABG in LMCA and 3 vessel disease has suggested that results with PCI are comparable to CABG especially in the subsets of isolated LMCA ir LMCA with single vessel disease (N Engl J Med. 2009;360:961-72). Another large observational study from 4 French centers involving 291 patients with unprotected distal left main lesions has reported excellent angiographic results and good mid term clinical outcomes with provisional side branch T stenting (Circulation 2009;119:2349-2356).
In this particular patient it was imperative that the RCA in stent restenosis was tackled first followed by cross-over stenting for the distal left main/ostial and proximal LAD lesions.
Conflict of Interest:
None