
To say that I was taken aback when Youtube pulled down my video entitled “ 2 Vaccine Shots Are A Must to Tackle the Delta/Indian Variant; But Till Fully Vaccinated Take Ivermectin”would be a gross understatement. I was actually nauseated by their mindless move. The video was less than 10 minutes. I was highlighting current data suggesting that a single vaccine shot would be highly inadequate in protecting against the Indian/Delta variant; I provided the link for the Public Health England preprint. The researchers point out that 2 shots would be far better but protection was still slightly compromised, it dropped from 66% to 59.8% with the ChAdOx1 (Covishield) and from 94% to 88% with the Pfizer mRNA vaccine.
I realised within minutes that there would be no one to champion my cause. All that bullshit about freedom of expression is just that ……loads of bull shit. I have waited for more than 48 hours but there has not been a whisper. I am not surprised one bit. We all have our own personal agendas whether we are politicians, bureaucrats, or journalists. Personal interest is not just of paramount interest, it is the only interest under the demeanour of integrity and single-minded purposefulness.
I have manifestly tread on some very important toes, which have cancelled my video with utmost immunity, like tossing out a fly in complete disregard. I was left with little choice, I uploaded my stuff on Vimeo and Bit Chute within hours. No one protested, there was not even a pretension. Are we servile people? Your guess is as good as mine.
My videos are a crystallisation of my thoughts, after practising clinical medicine for more than 40 years. I do not speak for any political party, NGO, or media outlet, and certainly not for any drug or vaccine company.
I also spoke of a research letter published a few days ago in The Lancet that underscored that there was a drop in neutralising capacity with the Pfizer vaccine against current variants of concern ( in 250 volunteers). Efficacy dropped 3 fold against the English/ Alpha variant and 6 fold against the Indian/ Delta variant. The conclusion drawn is that because of the reduction in neutralisation against emerging variants a third shot of vaccination should be considered. The letter bolsters this approach by mentioning that there was indeed a further drop in antibody activity when checked after 3 months of the second shot in 14 individuals.
I elaborated on the Indian/Delta variant by quoting reprints that concluded there reduced neutralisation activity by antibodies formed by the Pfizer vaccine. That the variant had added mutations in the 681, 452, 478 and 614 amino acid positions of the spike protein, which made the variant not only more transmissible but also more evasive against antibodies produced by natural infection or vaccines. The Indian/ Delta variant is dodgier.
I have been closely watching the behaviour pattern of this virus for the last one and a half years. I have observed both outpatients and patients admitted in Covid wards. I have scanned as many papers/ preprints/ news items on the Covid 19 virus that a single human can possibly can. The labour has been hard, rigorous and long. I have gone through all treatment trials of remdesivir, monoclonal antibodies, inhaled budesonide, fluvoxamine, barictinib, famotidine ,dexamethasone, tocilizumab, oxygen administration, interferon, lopinavir, chloroquine and of course ivermectin.
It is clinically obvious that, unlike last year, this time around entire households have got infected suggesting much greater infectivity of the Indian/Delta variant than the D614G variant operating last year. I do not need to be told by modellers in Warwickshire that a 40% increase in infectivity will result in 6000 admissions a day, and an increase in 50% transmissibility will force 10,000 hospital admissions a day. I and all of us in Delhi are aware that there have been many more hospital admissions this time around.
We were a very short time ago in an incredibly awful hole where there were neither hospitals beds nor oxygen supply. Everything was being sold in the black market, medicines and even hospital beds. There were reports of astronomical extraction of money for an ambulance or a taxi. A stunning and extraordinary display of greed atop the saddle of cruelty was on display.
Whether this variant was 40% more infective as mentioned by the English health secretary (health minister) or it was 30% to 100% more infective as uttered by professor “Lockdown” Ferguson mattered little to me. I knew the virus was far more infective this time.
Importantly, apart from being more infective, the wretched variant was clearly showing signs of greater virulence. This year, significantly more people were developing bilateral ground-glass opacities (GGO’s) and pneumonia. More patients were having a substantial drop in their oxygen levels. There has been greater mortality.
I have mentioned in the erased video about a preprint by the ICMR that has compared the pathology in hamsters infected by the Indian/Delta variant with hamsters infected by an earlier variant. The researchers have found a significant difference in viral loads in the lungs of the sacrificed animals as also disease in the lungs. Both viral quantity and lung pathology were considerably greater in the hamsters infected with the Indian/Delta variant. There was more congestion and haemorrhage accompanied by greater numbers of inflammatory cells and septal thickening in the lungs infected by the Indian/Delta variant.
So we have a situation around us. There is a variant of concern that is significantly more infective and virulent. These are not anecdotal reports or subjective impressions. A doctor in the US however well informed will just not have any clue of the clinical ramifications of the Indian/Delta variant or how to tackle it. This variant, let us face it, is deadlier.
No wonder the English are mulling on extending their lockdown by a fortnight or even a month. The Indian/Delta variant is the predominant virus in many parts of England. The English experts are aware of the greater virulence and infectivity of the Indian/Delta variant and hence do not want to take any chances.
The English health secretary announced in their parliament that of the 12300 infected people with the Indian/Delta variant, around 126 have been hospitalised. That is 1% hospitalisation in the Indian/Delta variant cohort. But there is one striking feature almost all infected patients have not been vaccinated. Only 3 patients (carrying the Indian/Delta variant) with both vaccination jabs have landed in the hospital.
The inference is simple and reassuring. Regardless of its infectivity or virulence 2 shots of vaccination ensure that only a minority will get hospitalised with the Indian/Delta variant.
I ended the video by stating the obvious; a single jab policy could be disastrous, 2 shots should be mandatory for protection against the current variant and future variants. I am still undecided about a third shot and would wait for more research to support such a protocol.
I also mentioned that a recent paper published in Nature informs us of plasma cells that burrow into the bone marrow and are capable of generating antibodies against the Covid19 virus for years.
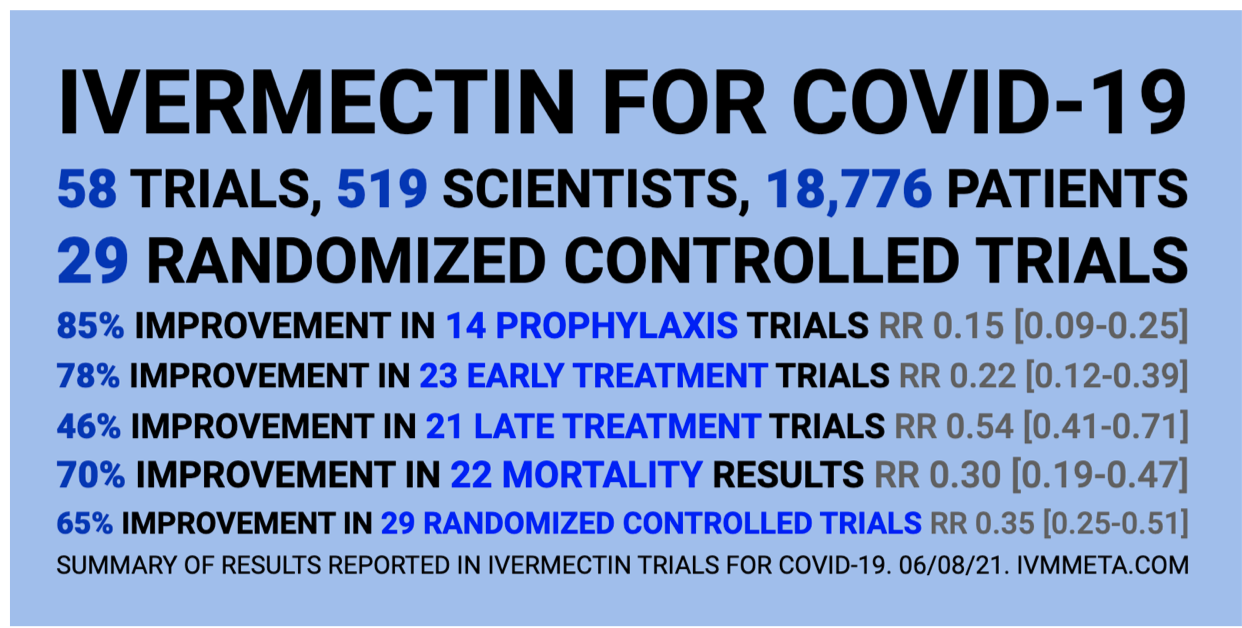
I also towards the end talked briefly about tablet ivermectin, which albeit has been used as anti-parasitic medicine for decades, has also been found to be exquisitely effective against early Covid 19 infection. I have used it in hundreds of patients with wonderful results. Not a single patient landed in hospital or died. Each one recovered, their ages ranged from 10 years to almost 80 years.
Ivermectin has also been very effective as prophylaxis in numerous randomised trials, in fact, a large comparative trial from AIIMS, Bhubaneshwar, has demonstrated an almost 90% reduction in infection in health care workers with just 2 tablets a month of ivermectin. To employ ivermectin for pre-exposure or post-exposure prophylaxis as being done in Uttar Pradesh would be a pragmatic and effective decision. Millions of people can be saved from being infected, especially in rural areas. The medicine is dirt cheap and easily available in the country.
So till the necessary proportion of people are infected in this country, once a week tablet ivermectin should be the way to go.
We just cannot rely on the advice provided by the WHO. The WHO has lurched from one faux pas to another in the last eighteen months. The mistakes have been awful and arbitrary.
I am compelled to mention a few.
Full-grown “scientists” in the WHO were sceptical that there would be effective immunity against Covid 19. This went against the grain of all common sense immunology/microbiology. It was being asserted (for the first time in human history) that the human body would be unable to make antibodies against the virus. When the expected backlash appeared WHO cunningly began to hint that antibodies would be temporary. We know now that not only is their robust antibody formation but reinfection after natural infection is very uncommon, and even if it does occur the intensity is considerably lessened.
The WHO took more than a year to revise its definition of the RT-PCR test. Finally, in the January of 2021 the WHO realised that the PCR was an aid to the diagnosis and not an end to itself. Also, it finally realised that there is something called the cycle threshold value (Ct). A high Ct value (used for almost a year in the West) is of little value. In fact the Car of Covid (currently under a lot of flak connected with the “lab leak” theory) Dr Anthony Fauci finally conceded that a Ct above 35 picks up only dead bases of the virus.
For some inexplicable reason, the WHO never cared to explain the importance of the Ct value with PCR testing. The change in approach became evident only this year. Very queer.
Another crucial change by the WHO has been the acceptance that the virus is “airborne”. Why should it take a bunch of full-grown “scientists” more than a year to realise that the virus is airborne and hence can hang in the air of a poorly ventilated room for almost 3 hours? That almost 99% of transmission in the case of Covid19, therefore, takes place indoors. Why did the esteemed scientists of the WHO not bother to employ palpable evidence spotted by most outside scientists? It is baffling and mind-boggling to say the least. So many millions infected and so many hundreds of thousands dead.
There are many more silly errors made by their Excellencies in the WHO but this one takes the cake. A huge uproar has been created regarding the origin of this virus. Suddenly Fauci looks extremely vulnerable and the knives are out for him. Undoubtedly the Yanks financed Chinese scientists to juice up coronaviruses and make them more deadly. They conveniently suspended “gain of function” experiments within their own shores but gave millions of dollars to Chinese scientists to pursue the lethal research.
The controversy is whether the virus came from a lab leak or whether it sprang from nature. If it came from a lab future research will be banned, but you and I know that such research will go on surreptitiously. If it came from nature we should expect another Pandemic in the not so distant future because there will be no change in human nature.
But I must get to the point and not digress from the principal issue. The WHO decided to send a commission to investigate the origin of this virus to Wuhan, China from where the Pandemic began sometime in 2019. Please read carefully, the WHO collects a small cohort of reputable scientists and slips in Peter Daszak of Eco Health Alliance fame also. The problem is, and this is a huge one, Peter is the guy who was the pipeline for the funding of the Wuhan Institute of Virology by the Americans ( NIH/ ministry of defence).
So we have the man who has been laundering money to the Chinese to specifically experiment on gain of function in coronaviruses to investigate whether the Chinese scientists were doing gain of function tests. Sounds bizarre but the entire world knows this. The entire Western media is bleating about this strange conflict of interest. I should rephrase ……glaring and brazen conflict of interest.

3 JUNE 2021
I bring out the chicanery of the WHO because I have a sneaking suspicion that it may have had a role in getting my video taken down. It cannot stand anyone mentioning ivermectin as a prophylactic or therapeutic against the Covid 19 virus.
8 JUNE 2021
If the reason for the cancellation was that I insisted on calling the variant the “Indian variant”…………it too is being downright absurd. Granted it has been given a new name, a Greek number “Delta” but the entire world still calls it the “Indian variant.” In fact, just about every newspaper in the UK has headlined the Indian variant with implications on their lockdown. One of their oldest and esteemed newspapers “The Times” calls it so, as also does the “Daily Mail” and also “Sky News.” The reason is that calling it the “Indian variant” is simpler for their readers to understand, there is no malice in it. British newspapers as also most English print media continues to term the B 1.617.2 as the “Indian Variant”, along with giving news of the “Kent” or “English variant .”

8 JUNE 2021
If I have been punished for making a purely scientific-educational video ( with the necessary links) on the Indian/Delta variant with the sole intent of providing information to the public, so be it. I have resolved NEVER to upload a video ever on YouTube. I have always been a clinician and a damn good one…. I will continue to be so. I shall also keep my eye on this virus.
More than one billion (one hundred crores) doses of ivermectin have been given in the last 30 years with not a single death. There are reports that more than 3 billion doses have been administered. Five to 10 tablets of ivermectin (of appropriate strength) taken over 5 days under the guidance of a physician cannot harm anyone, it is just impossible. There is absolutely no chance of getting a heart attack, cancer, respiratory failure, kidney or liver failure. On the contrary, there is every chance it will save you from going to a hospital and getting hooked to a ventilator. Again there is absolutely no probabilty of triggering a torsade de pointes or ventricular fibrillation or complete heart block. No chance of sparking restrictive, dilated or hypertrophic cardiomyopathy. No chance of a blood clot in the cavernous sinus of the brain or in a splanchnic vain. No probabilty whatsover of developing Bells palsy, transverse mylitis or the gullain barre syndrome. And no young boy will develop myocarditis within 4-5 days of finishinbg the short course.
The WHO analysis on ivermectin is not even worth writing about, it has cherry-picked data, arbitrarily downgraded the quality of evidence and come to the implausible conclusion that the drug is ineffective and worse not safe ( without a shred of evidence for the latter conclusion). There was no vote taken to make the final decision. Dodgy to say the least.

The paper that launched ivermectin was written by a group of brilliant scientists in Melbourne, Australia. This was the first research demonstrating ivermectin destroyed the Covid19 virus in 48 hours. Clinicians took note of this paper and the rest is history. Hundreds of thousands of lives have been saved across the planet. Interestingly the lead author of the first research paper is Dr Leon Caly whose mother comes from Kerala!
I have always maintained that this virus and this Pandemic are much bigger than any politics, religion or government, not to mention the WHO or Big Pharma. I may be a microscopic speck, smaller than the Covid19 virus (that is 60 to 140 nanometers in size) but I have never been petty. There is still a big heart, shaped by years of interval training.
YouTube has some ridiculous guidelines that are unleashed on a whim or something else.
