By Deepak Natarajan
Monday, November 22, 2010
Operator(s):
Deepak Natarajan
Affiliation:
Moolchand MedCity, New Delhi, India
Facility:
Department of Interventional Cardiology
Moolchand MedCity, New Delhi, India
History:
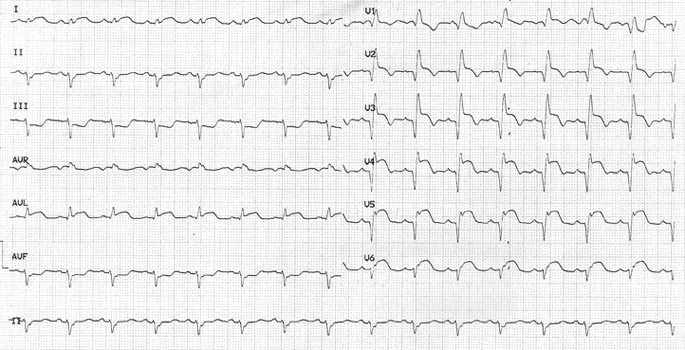
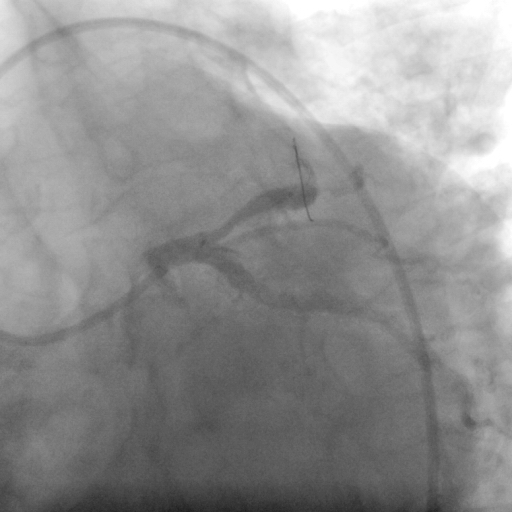
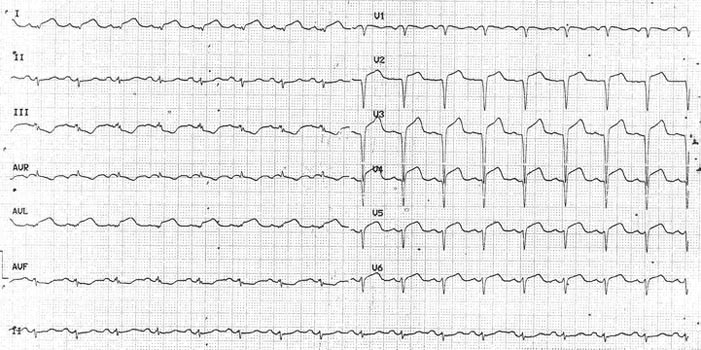
A 59 year old non diabetic, non hypertensive male was admitted for crushing chest pain radiating to both arms, accompanied by perspiration for the previous one hour. His EKG revealed extensive anterior myocardial infarction with bifascicular block (Figure 1).
{kind=link}
Angiography:
1) Left Main: normal
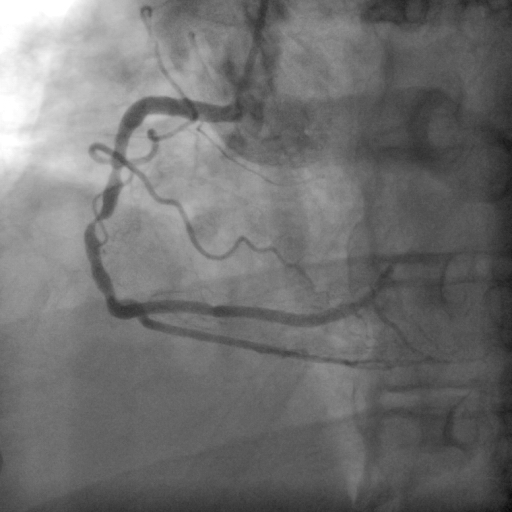
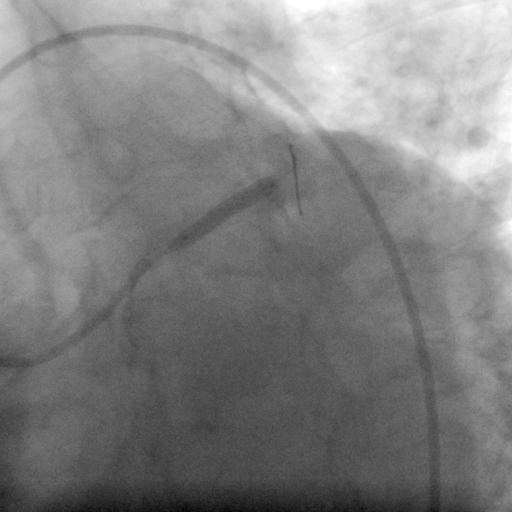
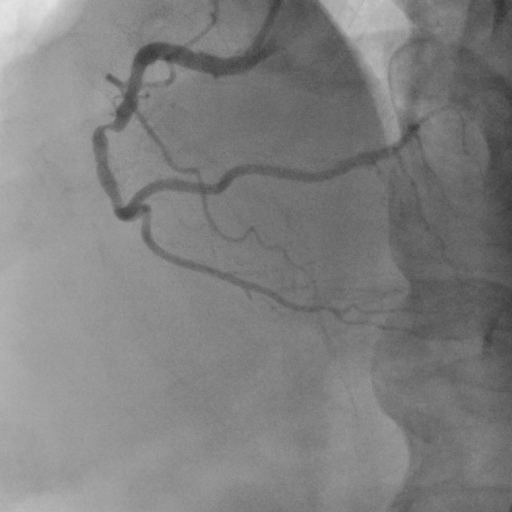
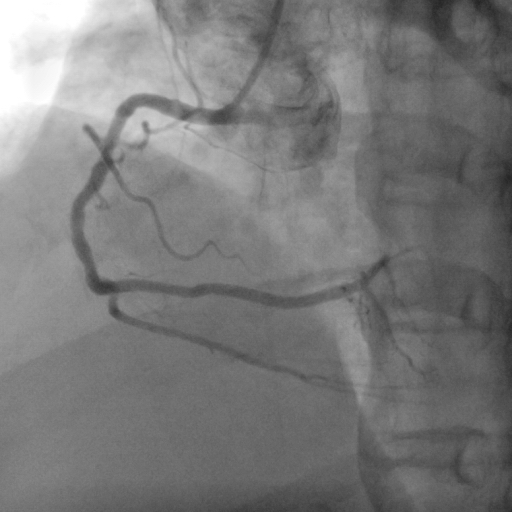
2) Left Anterior Descending Artery (LAD): 100% occlusion near ostium (Figure 2 and Figure 3)
3) Left Circumflex Artery (LCX): Mild disease
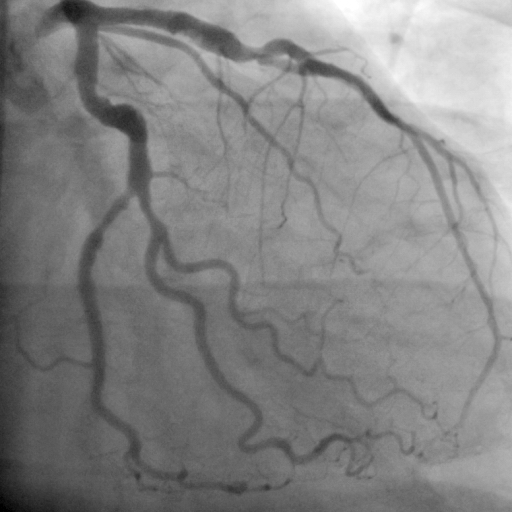
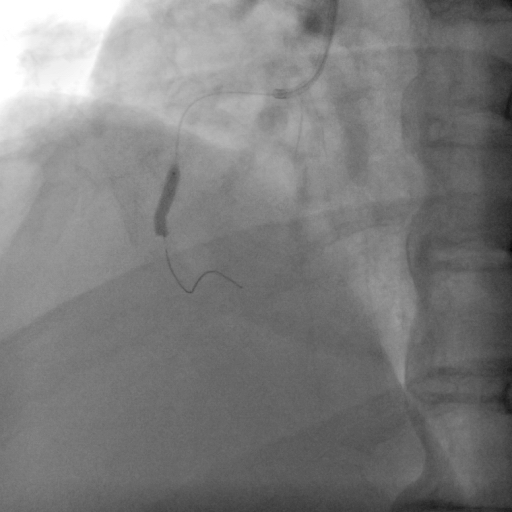
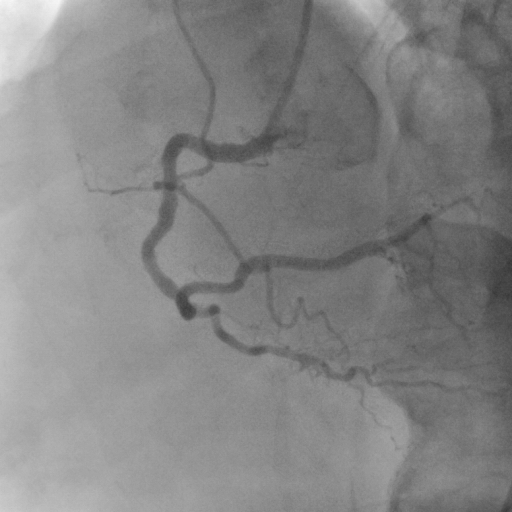
4) Right Coronary Artery (RCA): 85% mid vessel stenosis (Figure 4)
{kind=link}
{kind=link}
{kind=link}
Procedure:
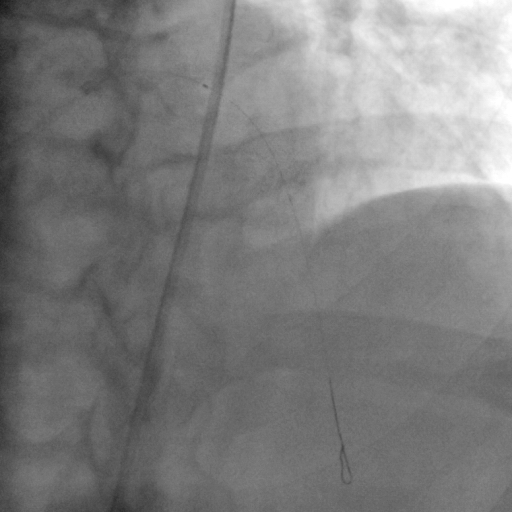
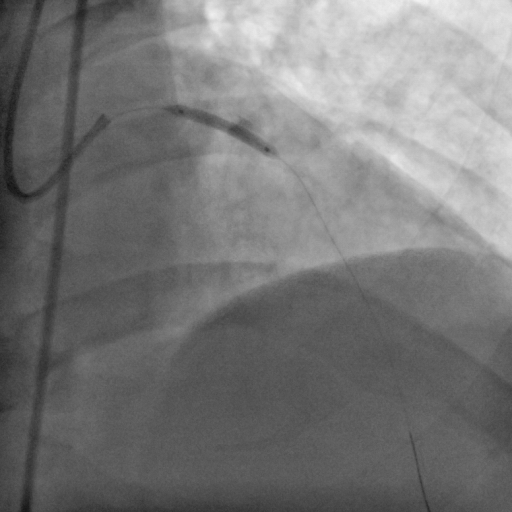
The left coronary artery ostium was engaged with a 6Fr left EBU guiding catheter and a 0.014″ BMW guidwire that was negotiated across the LAD occlusion. An intracoronary tirofiban bolus of 20mcg/Kg was administered, and repeated manual thrombus extraction was attempted using an Export catheter (Figure 5 and Figure 6). There was, however, little response in antegrade flow despite 6 attempts with the extraction catheter and repeat intracoronary tirofiban bolus of 10mcg/Kg. (Figure 7 and Figure 8). The patient was moved out of the cath lab into the coronary care unit, and intravenous tirofiban was infused at 0.15mcg/Kg/minute for the next 2 hours. The patient was wheeled back to the cath lab, and predilation was performed using 2.5x16mm and a 3x18mm balloons at 12atm (Figure 9and Figure 10). A long residual stenosis was apparent (Figure 11 and Figure 12), but reasonably brisk antegrade flow was achieved. Subsequently a 3.5x23mm everolimus-eluting stent (Xience) was deployed at 20atm (Figure 13). Angiography revealed TIMI 3 flow with minimal residual stenosis (Figure 14). The EKG revealed substantial improvement of the ST segments and disappearance of the bifascicular block (Figure 15).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
It was decided to tackle the RCA lesion on a later occasion because the patient was hemodynamically stable and the procedure had been prolonged. Hence, after 6 weeks his left coronary artery system appeared disease free (Figure 16), but the RCA stenosis persisted (Figure 17). The RCA was engaged with a 6 ]Fr JR guiding catheter with side holes. A 0.014″ BMW gjidewire was negotiated through the stenosis; and following predilation with a 2x10mm balloon, a 3×12 sirolimus-eluting stent (Yukon) was deployed at 18atm (Figure 18). There was no residual stenosis and TIMI 3 flow was obtained (Figure 19 and Figure 20).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Conclusion:
The patient received continuos IV tirofiban infusion subsequently for 18 hours. The patient was discharged on both occasions on aspirin, clopidogrel, cilostazol, atorvastatin, ramipril, and metoprolol.
Comments:
Primary angioplasty is the treatment of choice in the majority of patients. There are, however, instances when the operator is confronted with other affected arteries besides the infarct-related vessel. The majority of interventional cardiologists are currently of the opinion that in the absence of hemodynamic instability, it is prudent to stage the procedure in multivessel disease. The interval can extend from while the patient is still hospitalized to as late as 8 weeks. This patient presented with an extensive anterior myocardial infarction (accompanied by a bifascicular block on his EKG) that necessitated a prolonged procedure involving large quantities of contrast. The index procedure was itself staged because there was little-to-no response to repeated manual thrombus extraction and IC tirofiban. The patient, therefore, was treated after 2 hours of IV tirofiban infusion. A recent New York Sate Registry has reported that patients undergoing staged multivessel intervention within 2 months after STEMI, but not during the index procedure had significantly less mortality.
Conflict of Interest:
None